
19 August 2009 – Case of the Week #155
This email is only sent to subscribers. To subscribe or unsubscribe to this or our other email lists, email NatPernick@Hotmail.com, indicating subscribe or unsubscribe to [name of email]. Our email lists are:
- Case of the Week - 3 weeks/month
- Pathologist/PhD jobs - biweekly
- Other laboratory jobs - biweekly
- Pathology fellowships - biweekly
- Pathology website news - monthly
- Pathology new books - monthly
- The Detroit College Promise - the scholarship for Detroiters that we sponsor (monthly)
For our DermatologyOutlines.com website, we have these email lists:
- Dermatologist jobs / Practice openings - monthly
- Dermatology fellowships - monthly
- Dermatology website news - monthly
- Dermatology new books - monthly
Website News:
(1) If you have a Flickr account, you can upload gross, microscopic or other images directly to our Flickr group at http://www.flickr.com/groups/pathologyoutlines/. We will post a link to these images in the appropriate chapter of our online textbook, so pathologists and related personnel throughout the world can benefit from them. We will also list you as a contributor in our various news messages.
(2) We have updated the Smooth Muscle and Skeletal muscle sections of our Soft Tissue Tumors - Part 3 chapter, and are currently updating the Breast-malignant chapter.
To view the images or references in this Case of the Week, you must click on the links in blue. Links in green are to journals with free full text-no registration. You can also access these cases by visiting our Home Page, then click on the Case of the Week button on the left hand side.
Thanks to Dr. Asmaa Gaber Abdou, Menofiya University, Egypt, for contributing this case. To contribute a Case of the Week, email NatPernick@Hotmail.com with the clinical history, your diagnosis and diagnostic microscopic images (textbook quality) in JPG, GIF or TIFF format (send as attachments, we will shrink if necessary). Please include any other images (gross, immunostains, etc.) that may be helpful or interesting. We will write the discussion (unless you want to), list you as the contributor, and send you $35 (US dollars) by check or PayPal for your time after we send out the case. Please only send cases with high quality images and a diagnosis that is somewhat unusual (or a case with unusual features).
Case of the Week #155
Clinical History
An 18-year-old girl suffered from closely packed dark papules on her feet and legs since she was 6 years old. She now presented with new papules on her hands, extending to her arms. The papules were biopsied.
Micro images:
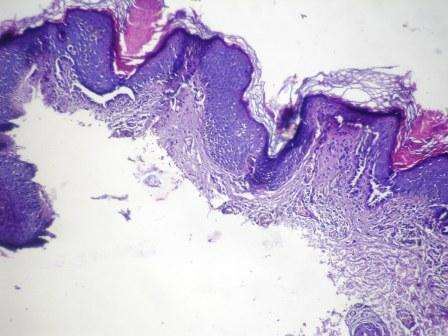
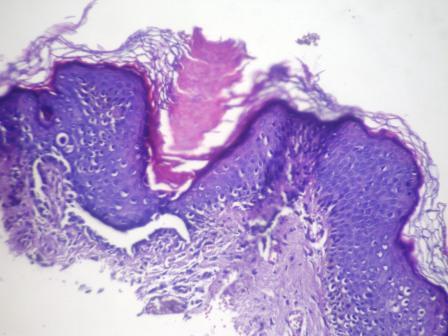
Low power
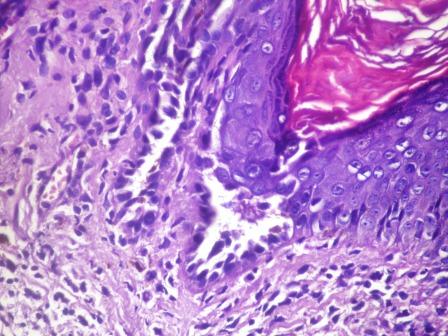

High power
What is your diagnosis?
Diagnosis:
Darier’s disease (Darier-White disease, keratosis follicularis)
Discussion:
Histologic examination of the papules revealed mild acanthotic epidermis with slight papillomatosis, hyperkeratosis and follicular plugging. Scattered dyskeratotic cells were present in the spinous layer. Cells displayed basophilic cytoplasm and round, pyknotic nuclei surrounded by clear halos (“corp ronds”), or elongated grain shaped nuclei (“grains”), a characteristic of Darier’s disease.
Darier’s disease is an autosomal dominant condition of the skin, nails and mucosal surfaces. It is caused by mutations in the ATP2A2 gene, encoding sarco-endoplasmic reticulum calcium pumping ATPase type 2 (SERCA2) (Cell Mol Life Sci 2008;65:205), which cause loss of adhesion between epidermal cells and abnormal keratinization. Patients usually present during their teenage years with dark, crusty, keratotic papules, sometimes filled with pus or accompanied by a strong, lingering odor. Lesions are exacerbated by heat and UV light. There is often no family history (J Eur Acad Dermatol Venereol 2005;19:114).
Treatment has limited success, and consists of topical and systemic retinoids. For acute flares, topical corticosteroids, cyclosporin and antibiotics have been used (Am J Clin Dermatol 2003;4:97).
The differential diagnosis includes:
• Acrokeratosis verruciformis - rare autosomal dominant disorder of keratinization; multiple flat, skin-colored keratotic wart-like lesions on dorsum of hands and feet; may be related to acral Darier’s disease but lacks dyskeratotic cells
• Familial benign pemphigus (Hailey-Hailey disease) - chronic autosomal dominant disorder with suprabasilar and widespread acantholysis
• Seborrheic dermatitis - papulosquamous disorder of sebum-rich areas of scalp, face and trunk; severity varies over time; also associated with Malassezia (a fungus); nonspecific histologic findings
• Transient acantholytic dermatosis (Grover’s disease) - pruritis is common; similar histologic findings of focal acantholysis, dyskeratosis and spongiosis
• Warty dyskeratoma - an isolated follicular lesion
Additional references: eMedicine, PathologyOutlines.com, Wikipedia, J R Soc Med 2003;96:439, Lever’s Histopathology of the Skin
Nat Pernick, M.D., President,
Kara Hamilton, M.S., Assistant Medical Editor
PathologyOutlines.com, Inc.
30100 Telegraph Road, Suite 408
Bingham Farms, Michigan (USA) 48025
Telephone: 248/646-0325
Email: NatPernick@Hotmail.com
Alternate email: NatPernick@gmail.com