
9 July 2009 – Case of the Week #151
This email is only sent to subscribers. To subscribe or unsubscribe to this or our other email lists, email NatPernick@Hotmail.com, indicating subscribe or unsubscribe to [name of email]. Our email lists are:
- Case of the Week - 3 weeks/month
- Pathologist/PhD jobs - biweekly
- Other laboratory jobs - biweekly
- Pathology fellowships - biweekly
- Pathology website news - monthly
- Pathology new books - monthly
- The Detroit College Promise - the scholarship program for Detroit Public School students that we sponsor (monthly)
For our DermatologyOutlines.com website, we have these monthly email lists:
- Dermatologist jobs / Practice openings
- Dermatology fellowships
- Dermatology website news
- Dermatology new books
Website News:
(1) Thanks to Jennifer Stumph, MD, Spectrum Health, for contributing images of schistosomiasis to the Parasitology chapter.
(2) We updated the Soft Tissue Tumors-Part 2 chapter (click here), which includes Fibrohistiocytic and Adipose tissue tumors. This chapter is in our new format, in which each topic is a separate page that is accessed by clicking on the link in the Table of Contents or Index. The pages now load faster, are easier to read with less scrolling, and include thumbnails for most of the 600+ images.
(3) We have started to apply our new format to the Stains chapter, and have extensively updated the topics on BG-8 (useful for mesothelioma) and D2-40 (a marker of lymphatics). For many stain topics, we now include a link to a company that supplies these markers (for example, Covance for these markers).
To view the images or references in this Case of the Week, you must click on the links in blue. Links in green are to journals with free full text-no registration. You can also access these cases by visiting our Home Page, then click on the Case of the Week button on the left hand side.
Thanks to Angel Fernandez-Flores, M.D., Ph.D., from Hospital El Bierzo and Clinica Ponferrada, Ponferrada, Spain, for contributing this case. To contribute a Case of the Week, email NatPernick@Hotmail.com with the clinical history, your diagnosis and diagnostic microscopic images (textbook quality) in JPG, GIF or TIFF format (send as attachments, we will shrink if necessary). Please include any other images (gross, immunostains, etc.) that may be helpful or interesting. We will write the discussion (unless you want to), list you as the contributor, and send you $35 (US dollars) by check or PayPal for your time after we send out the case. Please only send cases with high quality images and a diagnosis that is somewhat unusual (or a case with unusual features).
Case of the Week #151
Clinical History
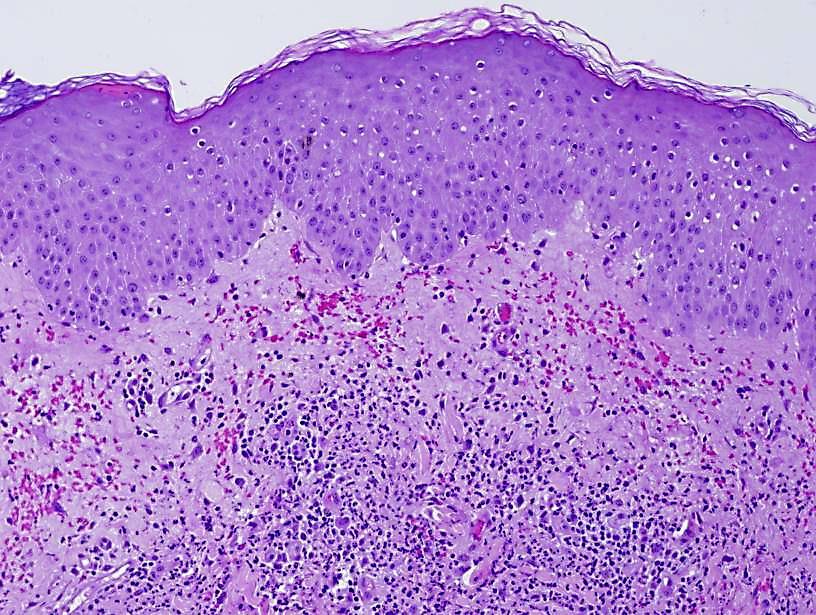
An 86-year-old man was diagnosed 10 months ago with atypical chronic myeloid leukemia, with lack of basophilia. The bone marrow aspirate was suggestive of non-progression to acute leukemia. He currently presented with more than five cutaneous lesions on his chest and back. They were red indurated papules, and the largest measured 1 cm in diameter.
{kind=link}
{kind=link}
{kind=link}
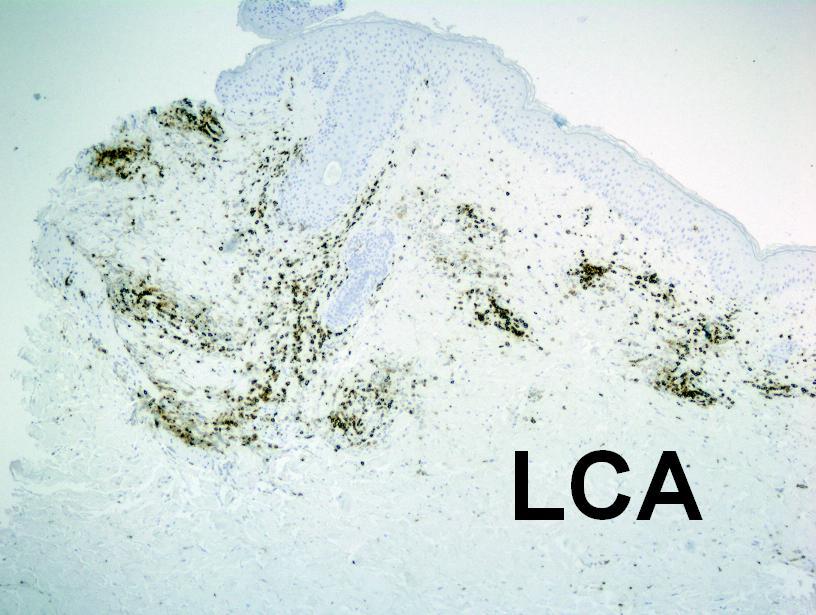
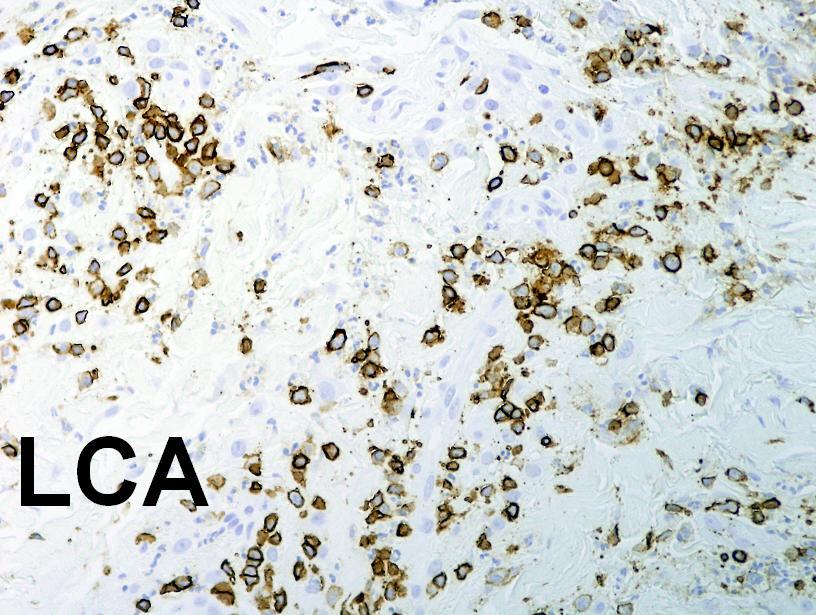
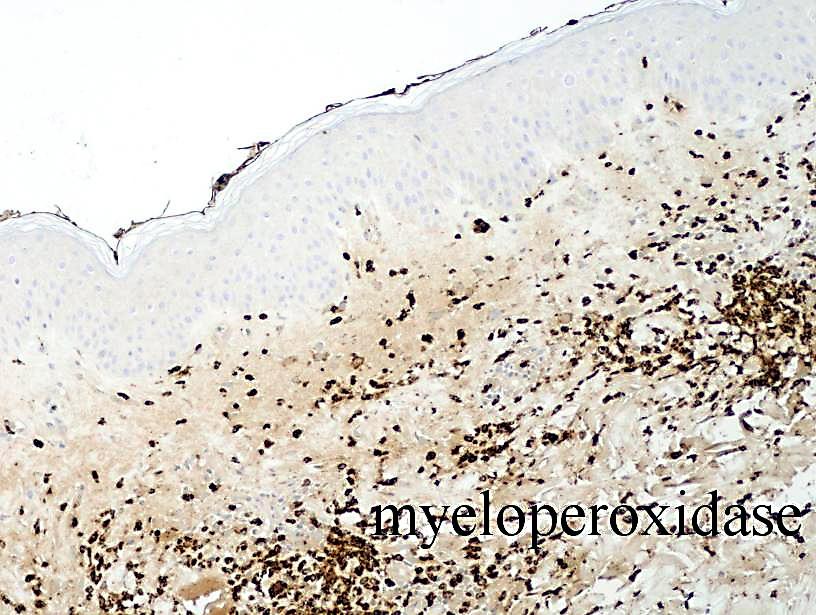
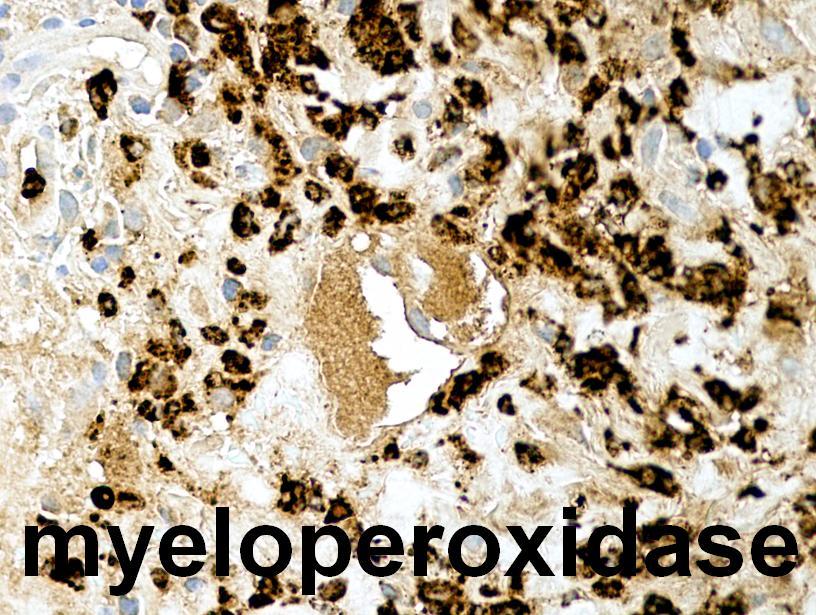
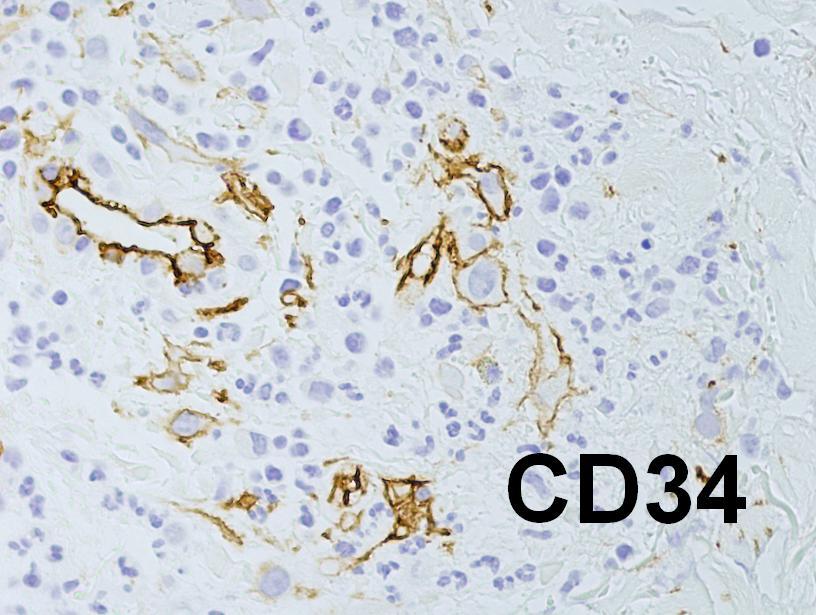
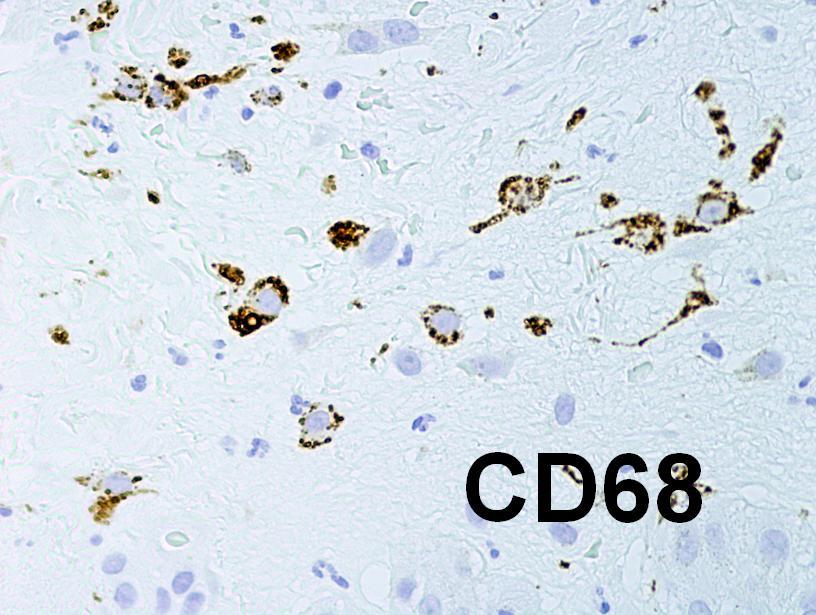
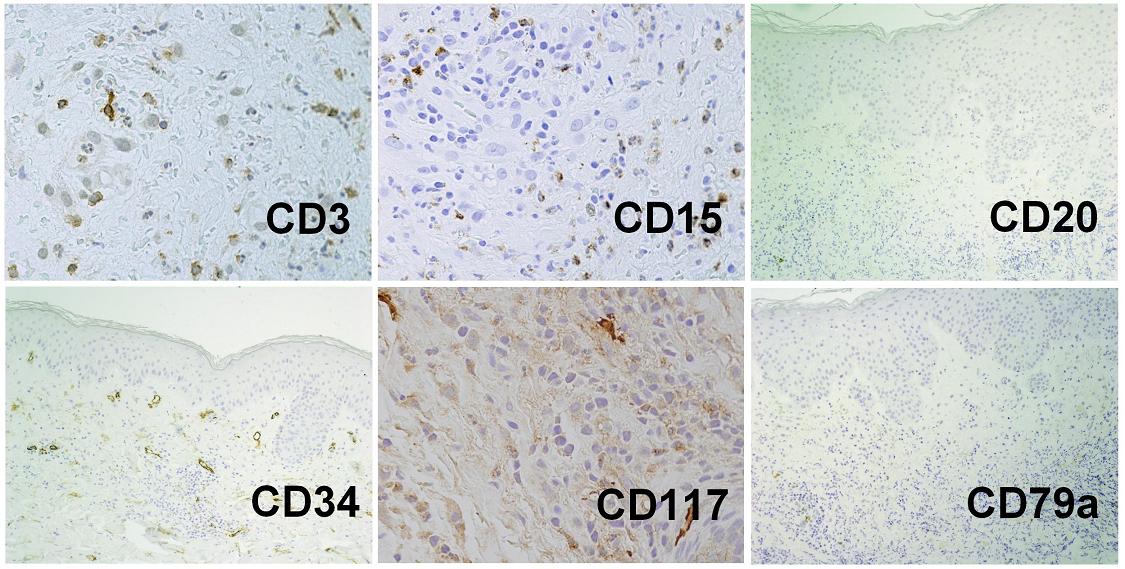
Immunohistochemistry: CD45/LCA #1; #2; Myeloperoxidase #1; #2; CD34; CD68; other CD markers
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
What is your diagnosis?
Diagnosis:
Leukemic vasculitis in the context of leukemia cutis, in a patient with atypical chronic myeloid leukemia.
Discussion:
Chronic myeloid leukemia (CML) is characterized by the t(9;22)(q34;q11) [Philadelphia chromosome], discovered in 1960 by Peter Nowell of the University of Pennsylvania and David Hungerford of the Fox Chase Cancer Center (J Natl Cancer Inst 1960;25:85), or by the fusion transcript of the ABL (#9q34) and BCR (#22q11) genes (Cell 1984;36:93).
Atypical CML is a myelodysplastic / myeloproliferative neoplasm that differs from classic CML by (a) the presence of marked granulocytic and multilineage dysplasia, (b) anemia and thrombocytopenia, (c) the lack of basophilia, and (d) the lack of a BCR-ABL fusion transcript by cytogenetics or RT-PCR (Eur J Haematol 2009 Jun 2 [Epub ahead of print]). Diagnosis requires RT-PCR to rule out a fusion gene, which may be present even with a normal karyotype (Hematol Oncol 2006;24:86). Atypical CML is also JAK2 negative (Leuk Res 2008;32:1931).
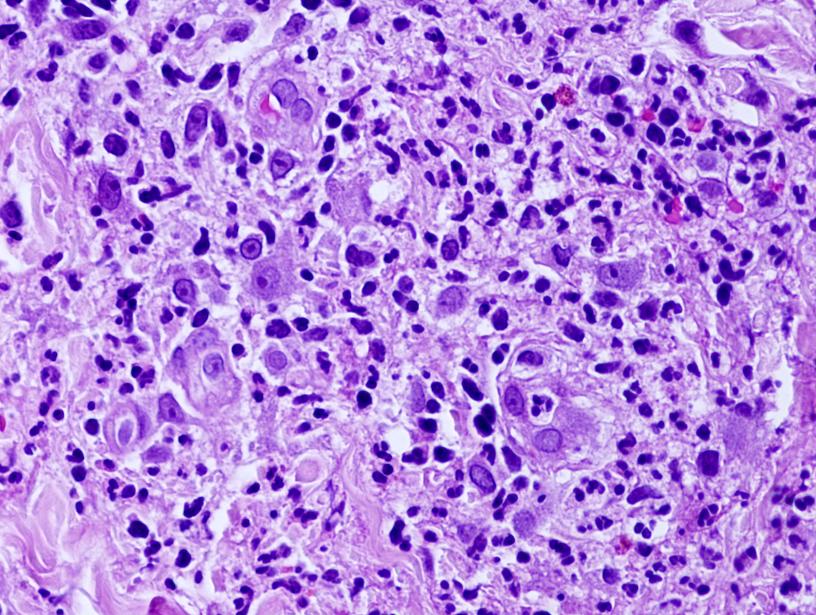
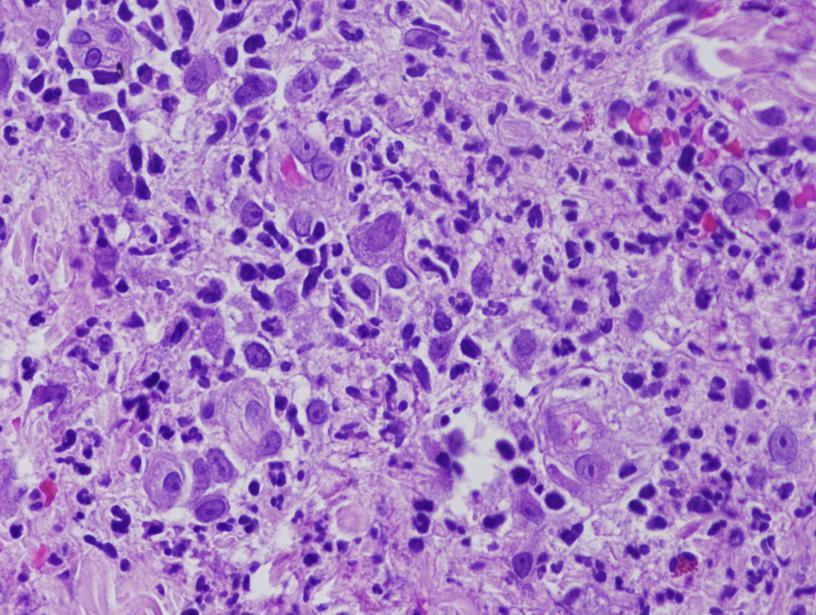
Leukemia cutis is the term used to describe neoplastic infiltration of the skin that arises in patients with systemic leukemias (Am J Clin Pathol 2008;129:130, Praxis 2002; 91:1071). Occasionally leukemia cutis precedes systemic leukemia and can be an early diagnostic factor (Clin Exp Dermatol 2004;29;468). Leukemia cutis tends to indicate an unfavorable prognosis (eMedicine), due to aggressive behavior and short survival (J Am Acad Dermatol 1999;40:966).
The infiltration of leukemic cells into the dermis or blood vessel walls is termed leukemic vasculitis (J Am Acad Dermatol 2009 May 28 [Epub ahead of print], Am J Clin Pathol 1997;107:637). It is often present in leukemia cutis (Br J Dermatol 2000;143:773). It is more aggressive than non-vasculitis leukemia cutis and is associated with a poorer prognosis. The differential diagnosis includes paraneoplastic vasculitis, often caused by antibiotics, cytokines or chemotherapeutic agents (Leuk Lymphoma 2000;40:105).
Nat Pernick, M.D., President
PathologyOutlines.com, Inc.
30100 Telegraph Road, Suite 408
Bingham Farms, Michigan (USA) 48025
Telephone: 248/646-0325
Email: NatPernick@Hotmail.com
Alternate email: NatPernick@gmail.com