
7 May 2009 Case of the Week #145
This email is only sent to subscribers. To subscribe or unsubscribe to this or our other email lists, send an email to NatPernick@Hotmail.com, indicating subscribe or unsubscribe to [name of email]. Our other Pathology email lists are:
● Pathologist/PhD jobs - biweekly
● Other laboratory jobs - biweekly
● Pathology fellowships - biweekly
● Pathology website news - monthly
● Pathology new books - monthly
● The Detroit College Promise - the charity we sponsor (monthly)

Attend the
27th Annual Summer Update in Clinical Immunology,
Microbiology and Infectious Diseases
July 13-17, 2009
Snow King Resort
Jackson, Wyoming (USA)
This review and update is intended to improve knowledge about the pathogenesis and clinical manifestations of infectious diseases, immunological mechanisms of disease and disease prevention, appropriate approaches to the diagnosis of infections and immunologic disorders, and utilization of the clinical microbiology and immunology laboratory including selection and interpretation of results.
For more information or to register, please click here.
Website News:
(1) We added a new article to our Management Page - Coding Prostate Saturation Biopsies, by Laura Edgeworth, PSA, LLC. Click here for the article or you can access the Management Page from the center section of our Home Page.
(2) We added a new article to our Management Page - Billing Contracts verses Managed Care Contracts, by Mick Raich, Vachette Pathology. Click here for the article or you can access the Management Page from the center section of our Home Page.
(3) Do you have good examples of Ovarian-nontumor pathology? Help your fellow pathologists worldwide by contributing these images to PathologyOutlines.com, where they will be viewed on a regular basis.
To view the images or references in this Case of the Week, you must click on the links in blue. Links in green are to journals with free full text-no registration. You can also access these cases by visiting our Home Page, then click on the Case of the Week button on the left hand side.
Thanks to Debra L. Zynger, MD and Jeffrey A. McDavit, MD, University of Pittsburgh Medical Center, Pittsburgh, PA, for contributing this case. To contribute a Case of the Week, email NatPernick@Hotmail.com with the clinical history, your diagnosis and diagnostic microscopic images (textbook quality) in JPG, GIF or TIFF format (send as attachments, we will shrink if necessary). Please include any other images (gross, immunostains, etc.) that may be helpful or interesting. We will write the discussion (unless you want to), list you as the contributor, and send you $35 (US dollars) by check or PayPal for your time after we send out the case. Please only send cases with high quality images and a diagnosis that is somewhat unusual (or a case with unusual features).
Case of the Week #145
Clinical History
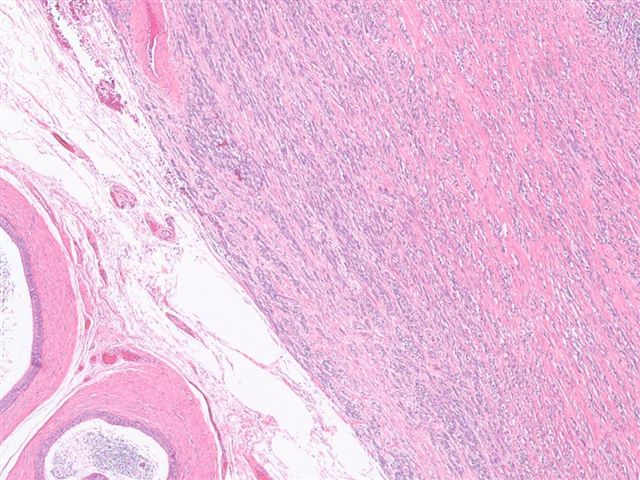
A 15-year-old boy presented with a paratesticular mass.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
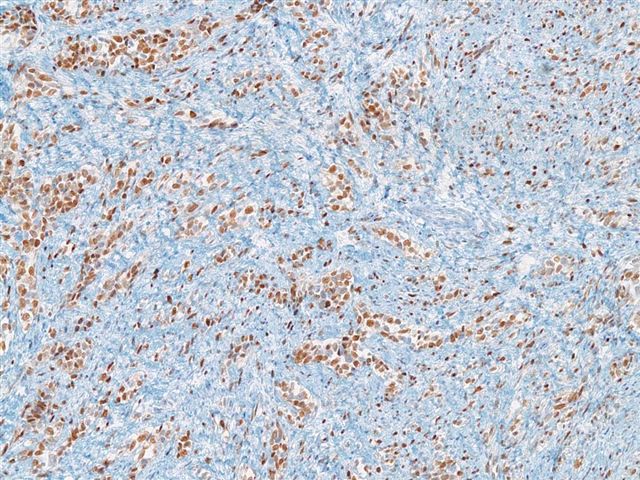
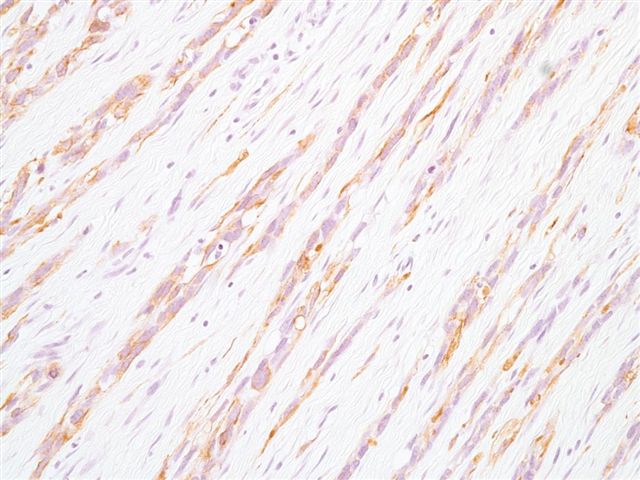
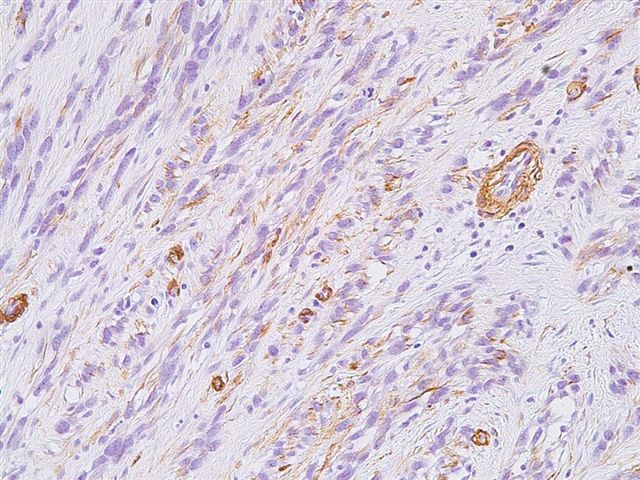
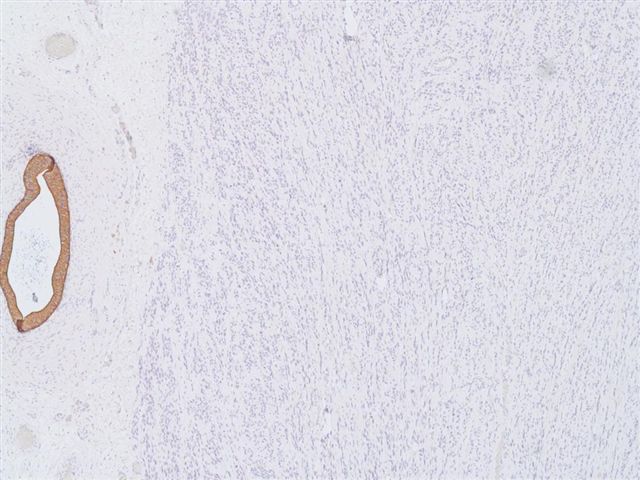
Stains: myogenin; desmin; SMA; AE1/AE3
{kind=link}
{kind=link}
{kind=link}
{kind=link}
What is your diagnosis?
Diagnosis:
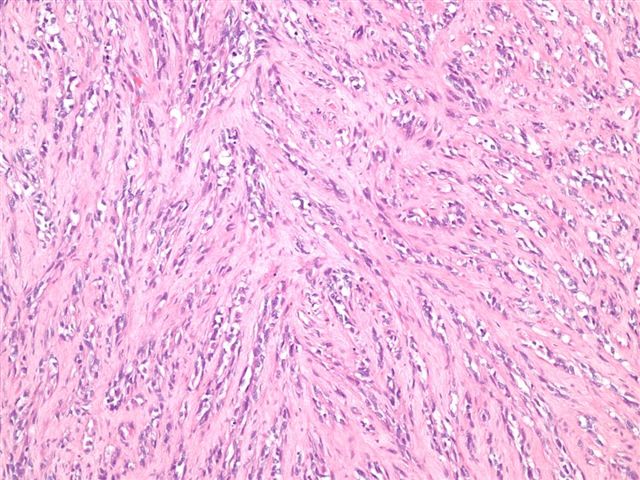
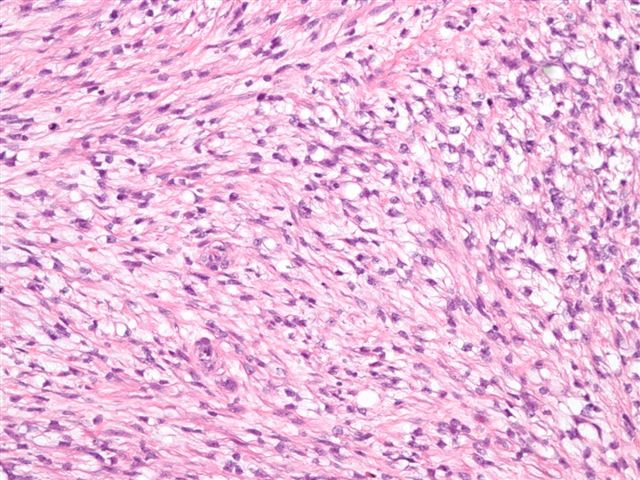
Spindle Cell Embryonal Rhabdomyosarcoma
Discussion:
Rhabdomyosarcomas are classified into embryonal, alveolar and pleomorphic types. Embryonal rhabdomyosarcoma can be further classified as spindle cell or botryoid subtypes.
Spindle cell rhabdomyosarcoma, first described in 1992, is most commonly found in the paratesticular region of young boys (Am J Surg Pathol 1992;16:229), although cases have also been described in adults (Am J Surg Pathol 2005:29:1106, Virchows Arch 2006;449:554). Grossly, the tumors are firm and fibrous, with a whorled cut surface resembling leiomyoma. Fine needle aspiration reveals numerous spindle cells and large fragments of cytoplasmic processes with cross-striations (Acta Cytol 2005;49:331). At excision, they are composed of a uniform proliferation of relatively bland, elongated spindle cells (at least 50% of tumor cells) with eosinophilic and fibrillar cytoplasm mimicking smooth muscle fibers. Nuclei are often elongated and vesicular. Scattered spindled or polygonal rhabdomyoblasts with brightly eosinophilic cytoplasm and pleomorphic nuclei are also present. Stains for desmin, myogenin, vimentin, myoD1, and smooth muscle actin are positive (Arch Pathol Lab Med 2006;130:1454). The tumor cells are negative for S100, keratin and caldesmon.
The differential diagnosis includes:
● fibrosarcoma - herringbone pattern, may have similar morphology but no rhabdomyoblasts, negative for skeletal muscle markers
● infantile fibromatosis - deep location, fascicles of spindle cells, no cross striations, no undifferentiated cells
● leiomyosarcoma - usually high grade, cigar shaped nuclei, no rhabdomyoblasts, often positive for caldesmon, negative for myoglobin
● neuromuscular hamartoma of soft tissue - usually age < 2 years, affects brachial plexus or sciatic nerve, multinodular growth with connective tissue separating nodules, no rhabdomyoblasts, muscular component is positive for desmin and muscle specific actin, neural component is positive for S100
● rhabdomyoma - benign tumor of skeletal muscle differentiation, no rhabdomyoblasts, no pleomorphism, no necrosis
Excision typically results in a good prognosis in children, but tumors in adults have a more aggressive course.
Additional references: Soft Tissue Tumor chapter of PathologyOutlines.com
Nat Pernick, M.D., President
PathologyOutlines.com, Inc.
30100 Telegraph Road, Suite 408
Bingham Farms, Michigan (USA) 48025
Telephone: 248/646-0325
Email: NatPernick@Hotmail.com
Alternate email: NatPernick@gmail.com