
25 February 2009 – Case of the Week #140
This email is only sent to subscribers. To subscribe or unsubscribe, email NatPernick@Hotmail.com, indicating subscribe or unsubscribe to Pathology Case of the Week. There is no charge. We do not sell, share or use your email address for any other purpose. We also have free email subscriptions for Pathologist/PhD jobs (biweekly), Other laboratory jobs (biweekly), Pathology fellowships (biweekly), Pathology fellowships (biweekly), Pathology website news (monthly), Pathology new books (monthly) and The Detroit College Promise-the charity which we sponsor (monthly). Email us to subscribe.
To view the images or references, you must click on the links in blue. Links in green are to journals with free full text-no registration. You can also access these cases by visiting our Home Page, then click on the Case of the Week button on the left hand side.
Thanks to Dr. Julia Braza, Beth Israel Deaconess Medical Center, Boston, Massachusetts (USA), for contributing this case. To contribute a Case of the Week, email NatPernick@Hotmail.com with the clinical history, your diagnosis and diagnostic microscopic images in JPG, GIF or TIFF format (send as attachments, we will shrink if necessary). Please include any other images (gross, immunostains, etc.) that may be helpful or interesting. We will write the discussion (unless you want to), list you as the contributor, and send you $35 (US dollars) by check or PayPal for your time after we send out the case. Please only send cases with high quality images and a diagnosis that is somewhat unusual (or a case with unusual features).
Case of the Week #140
Clinical History
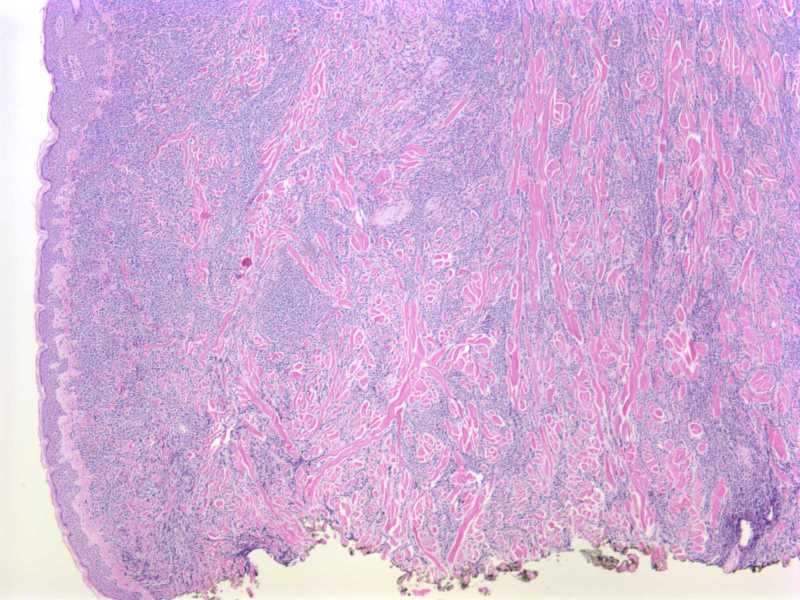
A 68 year old woman with a history of AML presented with a five month history of progressive eruption of violaceous firm nodules in the umbilicus, groin, trunk and scalp.
A left breast punch biopsy was performed.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
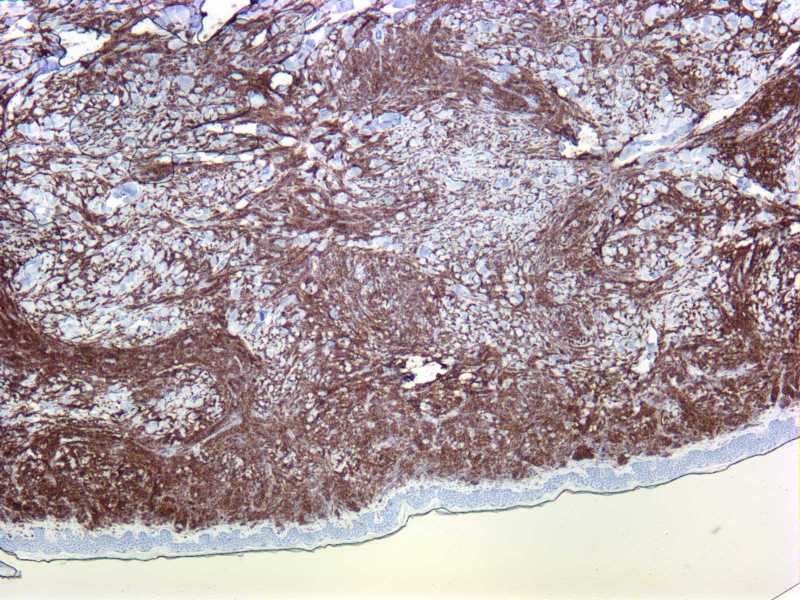
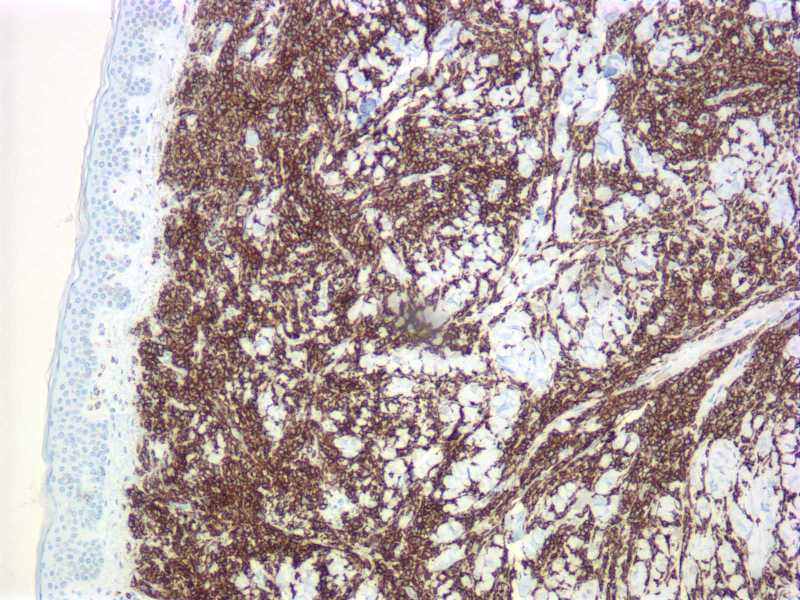
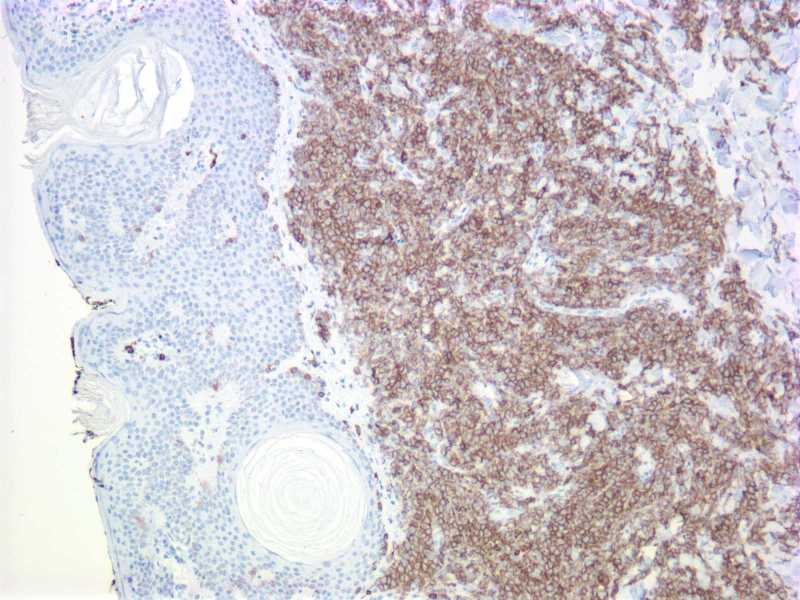
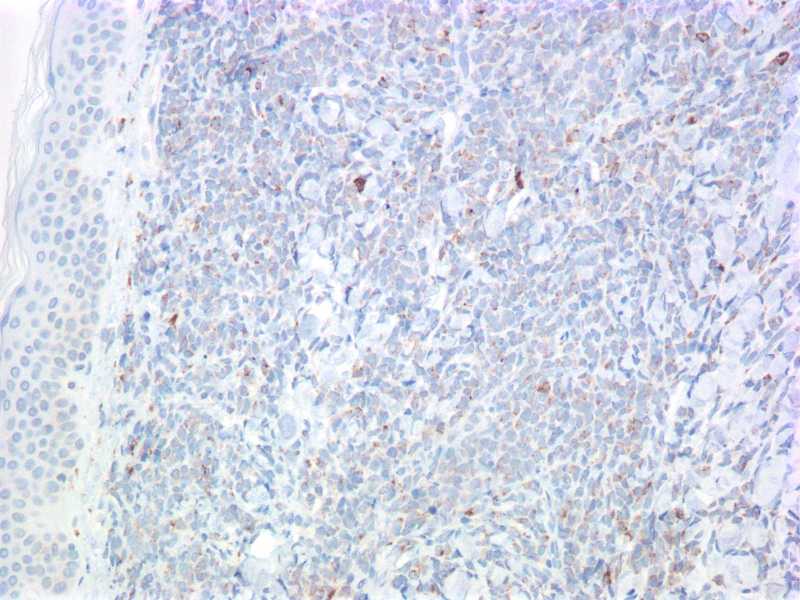
Stains: CD45; CD43; CD117; CD68
{kind=link}
{kind=link}
{kind=link}
{kind=link}
What is your diagnosis?
Diagnosis:
Leukemia cutis
Discussion:
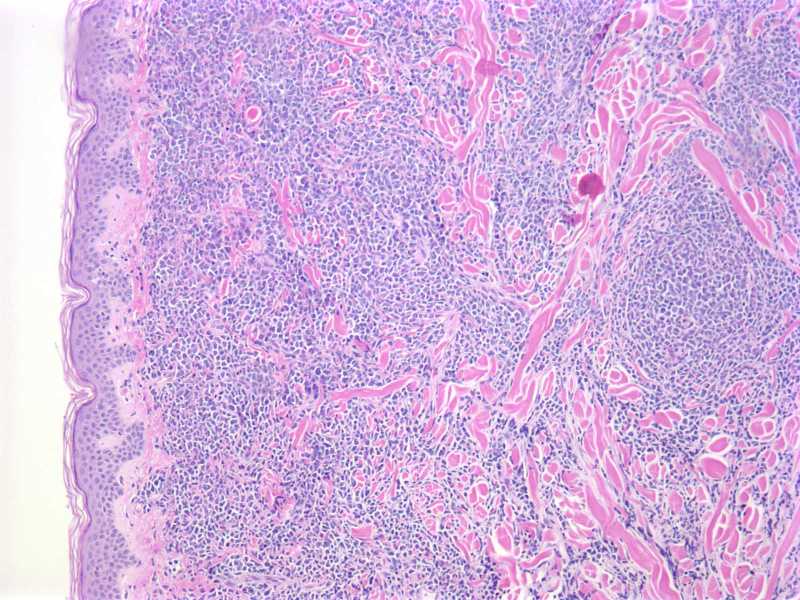
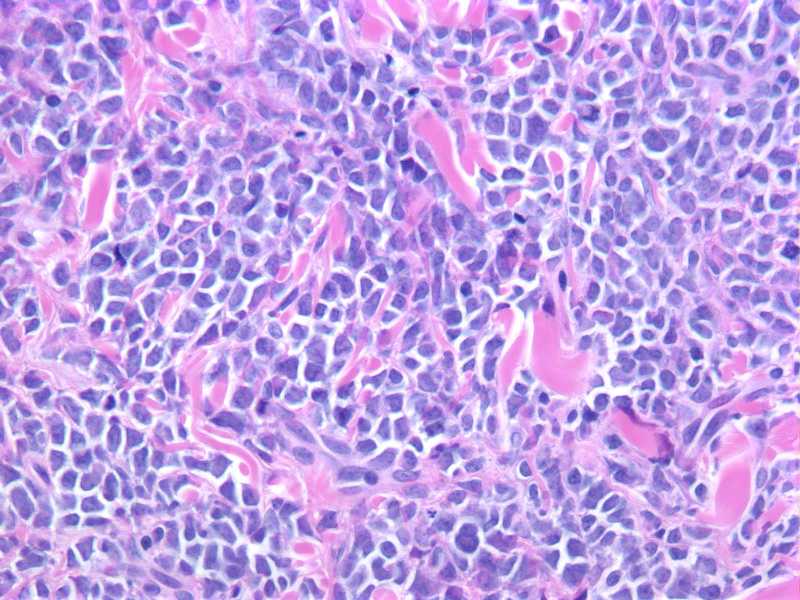
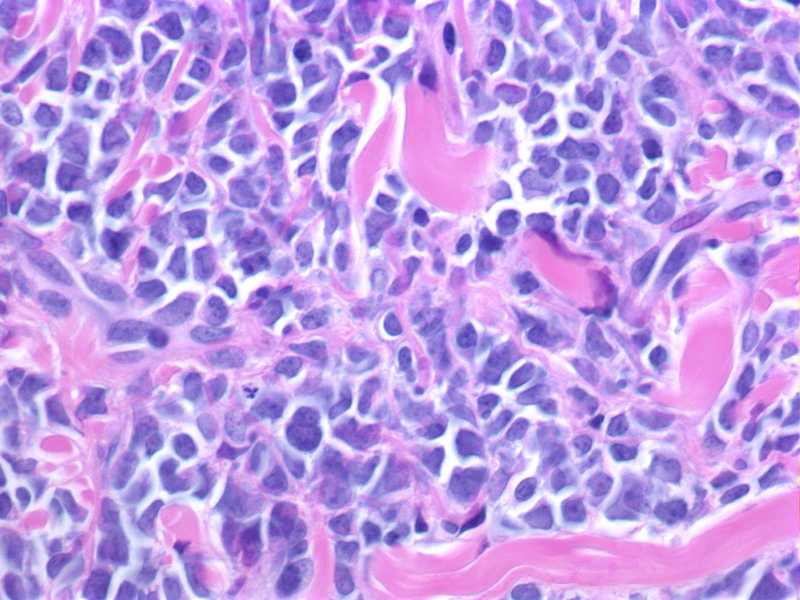
The dermis and superficial subcutaneous fat are diffusely infiltrated by a monotonous population of large cells with a high nuclear to cytoplasmic ratio, round to slightly irregular nuclear contours, finely dispersed chromatin and prominent nucleoli. The tumor cells are diffusely immunoreactive for CD45, CD117 and CD43, with focal expression of CD68. Myeloperoxidase (not shown) highlights a small subset of tumor cells. The cells are negative for CD34, TdT, CD20, bcl-1, and CD56. CD3 and CD4 (not shown) highlight scant, admixed T-lymphocytes.
Overall, the morphologic and immunophenotypic findings are consistent with tissue infiltration by acute myelogenous leukemia. The prior AML subtype is unknown.
Leukemia cutis includes cutaneous manifestations of any type of leukemia. It can be difficult to clinically distinguish from other skin lesions. Patients usually have preexisting systemic leukemia, but occasionally skin involvement precedes bone marrow or peripheral blood involvement (Am J Clin Pathol 2008;129:130)
Myeloid leukemia with monocytic differentiation more commonly involves the skin than other types of myeloid leukemia. It may also have an accompanying vasculitis (Am J Clin Pathol 1997;107:637). CD68 and lysozyme immunostains are sensitive for monocytes/macrophages, although not specific (J Cutan Pathol 2008;35:180)
Leukemia cutis is associated with aggressive behavior and short survival (J Am Acad Dermatol 1999;40:966). Treatment is systemic chemotherapy directed at eradicating the leukemic clone.
Additional references: eMedicine
Nat Pernick, M.D., President
PathologyOutlines.com, Inc.
30100 Telegraph Road, Suite 408
Bingham Farms, Michigan (USA) 48025
Telephone: 248/646-0325
Email: NatPernick@Hotmail.com
Alternate email: NatPernick@gmail.com