
19 February 2009 – Case of the Week
#139
This email is only sent to
subscribers. To subscribe or
unsubscribe, email NatPernick@Hotmail.com,
indicating subscribe or unsubscribe to Pathology Case of the Week. There is no charge. We do not sell, share or use your email
address for any other purpose. We also
have free email subscriptions for Pathologist/PhD jobs (biweekly), Other
laboratory jobs (biweekly), Pathology fellowships (biweekly), Pathology website
news (monthly) and Pathology new books (monthly). Email us to subscribe.
To view the images or references,
you must click on the links in blue. Links in green are to journals with free full text-no
registration. You can also access these
cases by visiting our Home Page, then click on the Case of the
Week button on the left hand side.
Thanks to Dr. Aparna Mahajan,
Case of the Week #139
Clinical
History
A 53 year old man with bipolar
disorder experienced sudden cardiac arrest.
Findings at autopsy included coronary artery disease and bilateral
symmetrical enlargement of the thyroid (30g).
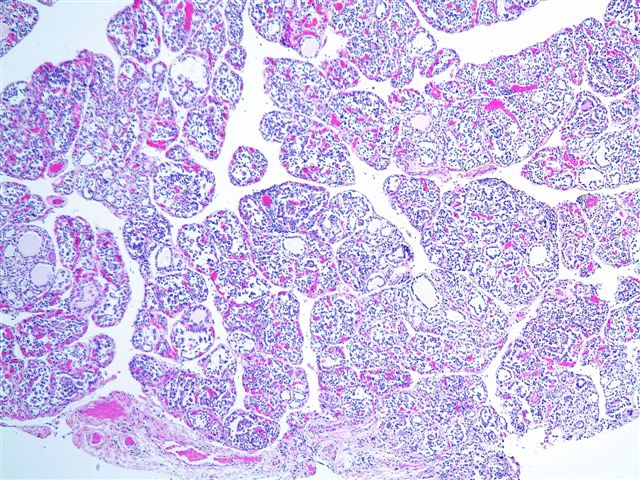
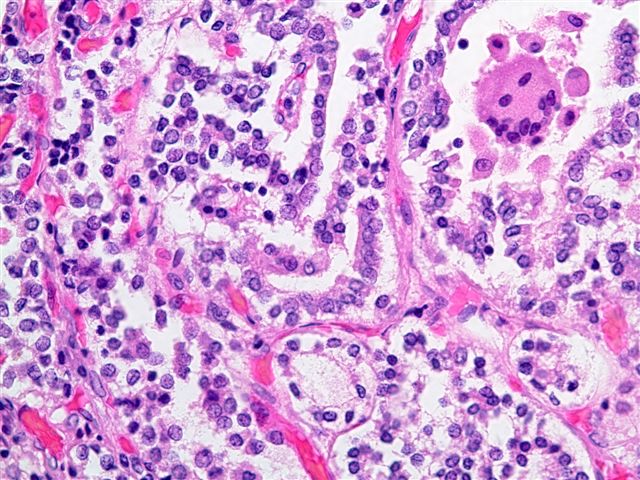
Micro images: #1; #2; #3; #4; #5; #6
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
What is your diagnosis?
Diagnosis:
Lithium induced thyroiditis
Discussion:
The patient had a history of lithium
use.
Most follicles are small and
atrophic with minimal colloid. The
follicles contain desquamated follicular cells, macrophages and multinucleated
giant cells. Some giant cells contain
birefringent crystals consistent with calcium oxalate. These findings are compatible with lithium
induced thyroid dysfunction (J Clin Pathol 1995;48:582). Lithium directly damages thyroid follicular cells, which
releases thyroglobulin, which may be hydrolyzed to thyroxine, causing
hyperthyroidism.
Psychotropic drugs such as lithium
have arrhythmogenic effects which can be exacerbated with preexisting cardiac disease,
and can cause sudden death (Can J Psychiatry 2004;49:100). However, there
was no evidence of arrhythmia in this case.
The differential diagnosis includes
lithium induced autoimmune thyroiditis, which has prominent lymphocytic
inflammation, lymphoid follicles and Hürthle cells (J Clin Pathol 1997;50:172), which were not
seen in this case.
Nat Pernick, M.D., President
PathologyOutlines.com, Inc.
Bingham Farms,
Telephone: 248/646-0325
Email: NatPernick@Hotmail.com
Alternate email: NatPernick@gmail.com