
22 January 2009 Case of the Week #137
This email is only sent to subscribers. To subscribe or unsubscribe, email NatPernick@Hotmail.com, indicating subscribe or unsubscribe to Pathology Case of the Week. There is no charge. We do not sell, share or use your email address for any other purpose. We also have free email subscriptions for Pathologist/PhD jobs (biweekly), Other laboratory jobs (biweekly), Pathology fellowships (biweekly), Pathology website news (monthly) and Pathology new books (monthly). Email us to subscribe.
To view the images or references, you must click on the links in blue. Links in green are to journals with free full text-no registration. You can also access these cases by visiting our Home Page, then click on the Case of the Week button on the left hand side.
Please tell your colleagues, residents, fellows, pathology assistants and laboratory personnel about our website. Please also let us know if you have any suggestions for improvement in 2009.
Thanks to Dr. David Cohen, Herzliyah Medical Center, Israel for contributing this case. To contribute a Case of the Week, email NatPernick@Hotmail.com with the clinical history, your diagnosis and diagnostic microscopic images in JPG, GIF or TIFF format (send as attachments, we will shrink if necessary). Please include any other images (gross, immunostains, etc.) that may be helpful or interesting. We will write the discussion (unless you want to), list you as the contributor, and send you $35 (US dollars) by check or PayPal for your time after we send out the case. Please only send cases with high quality images and a diagnosis that is somewhat unusual (or a case with unusual features).
Case of the Week #137
Clinical History
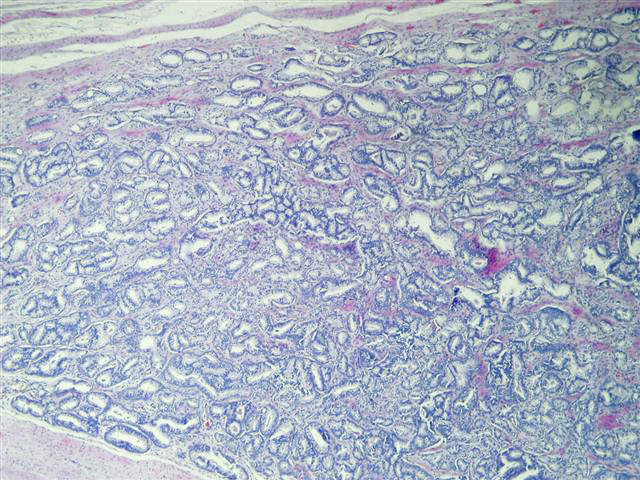
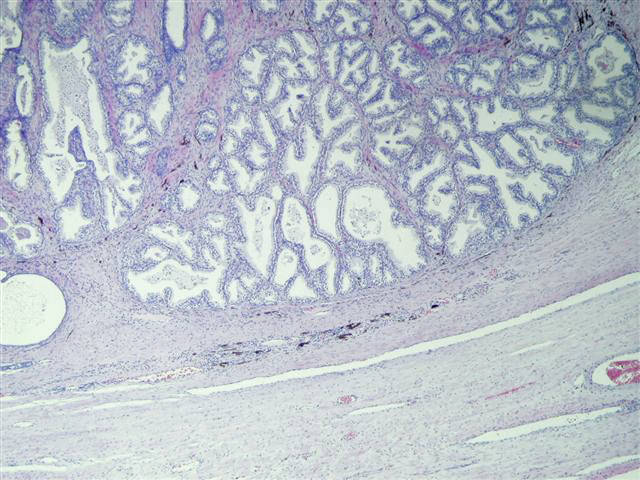
A 72 year old man had a radical prostatectomy for prostatic adenocarcinoma.
Micro images: #1; #2; #3; #4; #5; #6
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
What is your diagnosis?
Diagnosis:
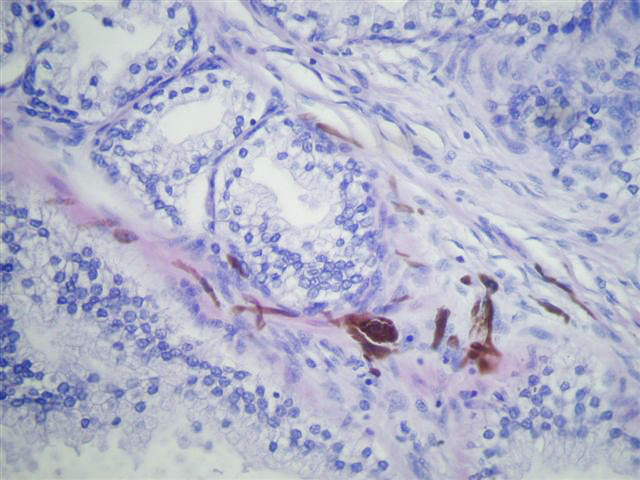
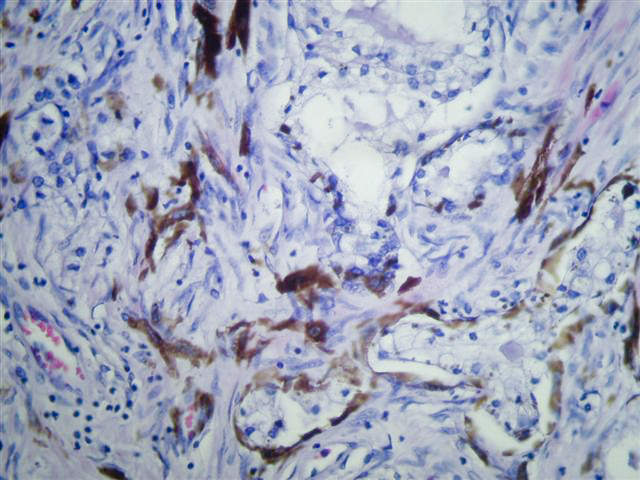
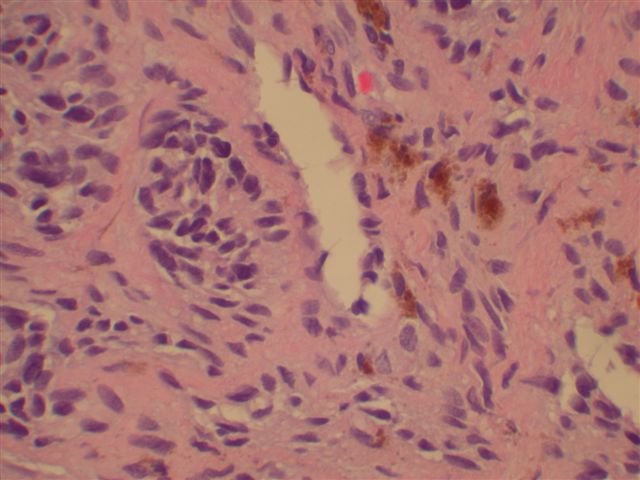
Prostatic adenocarcinoma (Gleason score 3+3 = 6)
Prostatic melanosis
Discussion:
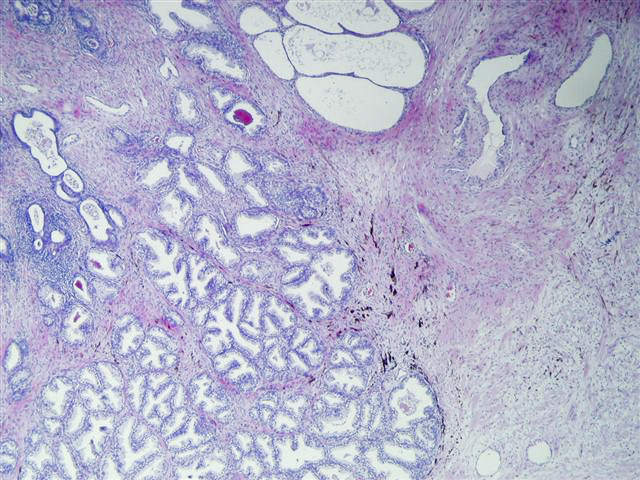
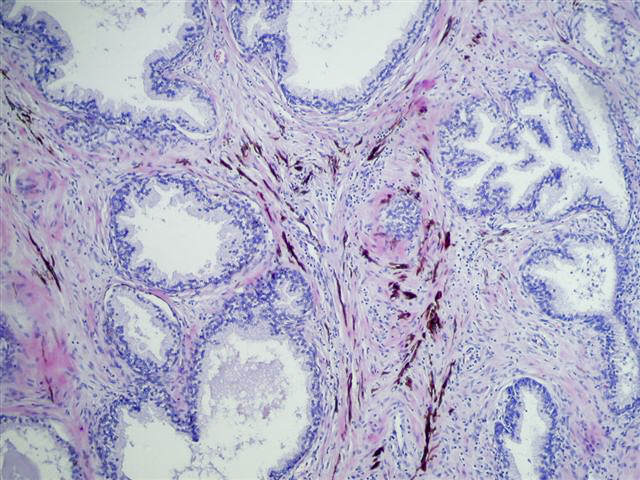
Prostatic melanosis is the finding of melanin within prostatic stromal melanocytes and glandular cells. The stromal melanocytes are believed to transfer melanin to the epithelial cells (Am J Clin Pathol 1988;90:530). Prostatic melanosis may be an isolated finding, associated with blue nevus (Eur Urol 1992;22:339) or associated with other prostatic pathology such as adenocarcinoma, as in this case.
The differential diagnosis includes lipofuscin pigment and blue nevus. Although lipofuscin is characteristic of ejaculatory ducts and seminal vesicles, it is also found in prostatic epithelium (Am J Surg Pathol 1994;18:446, Mod Pathol 1996;9:791). It is composed of golden yellow-brown to gray-grown granules (lipofuscin in hepatocytes). It stains with PAS-diastase, Congo Red, Luxol fast blue, Oil red O and Ziehl-Neelsen. Both lipofuscin and melanin stain with Fontana-Masson stain, but lipofuscin is S100 negative.
Blue nevus exhibits spindled stromal cells with marked melanin deposition (cellular blue nevus in skin). Nevus cells without pigment are usually present.
{kind=link}
There is no clinical significance to the presence of melanosis in the prostate.
Nat Pernick, M.D., President
PathologyOutlines.com, Inc.
30100 Telegraph Road, Suite 408
Bingham Farms, Michigan (USA) 48025
Telephone: 248/646-0325
Email: NatPernick@Hotmail.com
Alternate email: NatPernick@gmail.com