
7 November 2008 Case of the Week #134
To view the images or references, you must click on the links in blue. Links in green are to journals with free full text-no registration. You can also access these cases by visiting our Home Page, then click on the Case of the Week button on the left hand side.
This email is sent only to subscribers. To subscribe or unsubscribe, email NatPernick@Hotmail.com, indicating subscribe or unsubscribe to Pathology Case of the Week. There is no charge. We do not sell, share or use your email address for any other purpose. We also have free email subscriptions for Pathologist/PhD jobs (biweekly), Other laboratory jobs (biweekly), Pathology website news (monthly) and Pathology new books (monthly). Email us to subscribe.

23rd Annual Park City Surgical Pathology Workshop
This 20-hour workshop is designed for the pathologist, clinician, and oncology specialist, focusing on surgical pathology, cytopathology, and hematopoietic pathology.
Short lectures and case-oriented discussions will include in-depth reviews of diagnostic anatomic pathology, insight into difficult differential diagnoses, use of immunohistochemistry and new technology to improve diagnosis.

Participants at the 23rd Annual Surgical Pathology Workshop will be asked to examine microscopic images and formulate a diagnosis and patient management strategy. The faculty pathologist will then discuss the diagnosis, differential diagnosis, patient management, and other pertinent features. Cases will be selected to represent common and/or difficult diagnostic problems. Held at The Canyons in Park City, Utah. Click here for our website.
How can you learn about new fellowship openings? We have a new email list sent out every two weeks, listing the new fellowships posted at our website. To subscribe, email NatPernick@Hotmail.com with subscribe to Path fellowships email in the subject line.
Please visit our Management Page (under Clinical Pathology topics in the center section of our Home Page, or click here), to read the new article, The Tangled Web of Claim Payments - How Managed Care Contracts Kill Your Revenue. The informative articles on the Management Page are written exclusive for our website.
We thank Dr. Angela Bohlke, Tulane University Hospital, New Orleans, Louisiana (USA) for contributing this case. To contribute a Case of the Week, email NatPernick@Hotmail.com with the clinical history, your diagnosis and diagnostic microscopic images in JPG, GIF or TIFF format (send as attachments, we will shrink if necessary). Please include any other images (gross, immunostains, etc.) that may be helpful or interesting. We will write the discussion (unless you want to), list you as the contributor, and send you $35 (US dollars) by check or PayPal for your time after we send out the case. Please only send cases with high quality images and a diagnosis that is somewhat unusual (or a case with unusual features).
Case of the Week #134
Clinical History
A 10 year old girl presented with abdominal pain and anorexia. CT scan showed a 15 cm heterogeneous liver mass. Following rupture of the mass into the peritoneum, she was taken urgently to the operating room exploration and ultimately resection.
Gross image: #1
{kind=link}
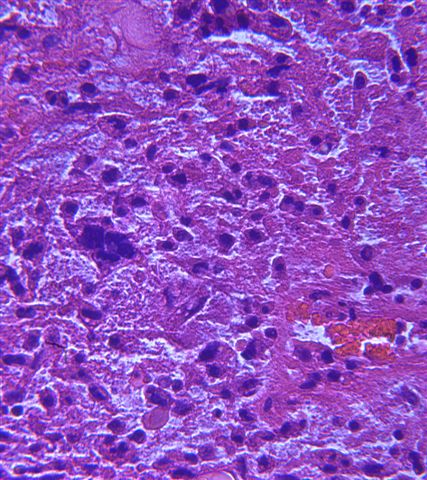
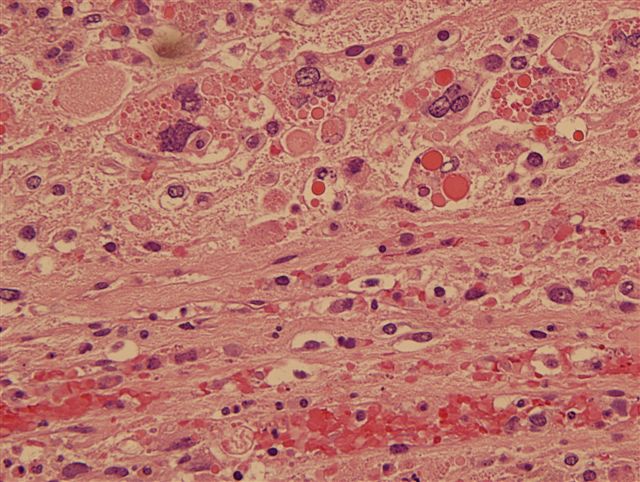
Micro images: #1; #2; #3; #4; #5; PAS diastase;
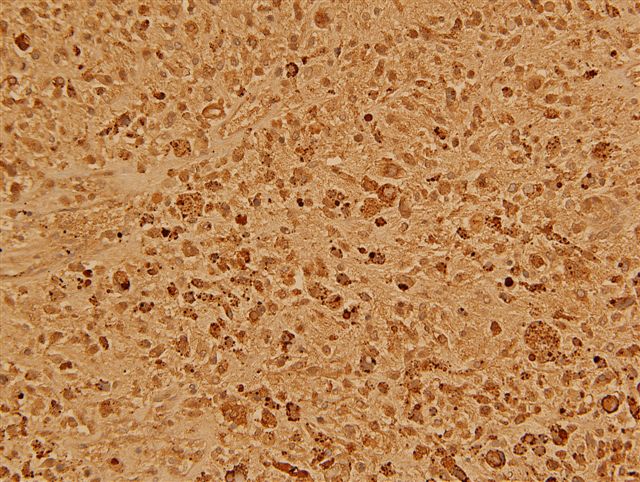
alpha-1-antitrypsin
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
What is your diagnosis?
Diagnosis:
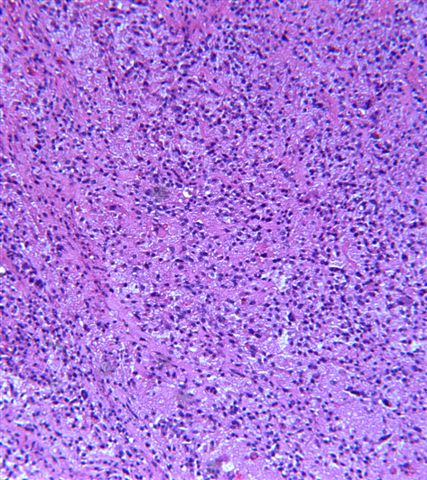
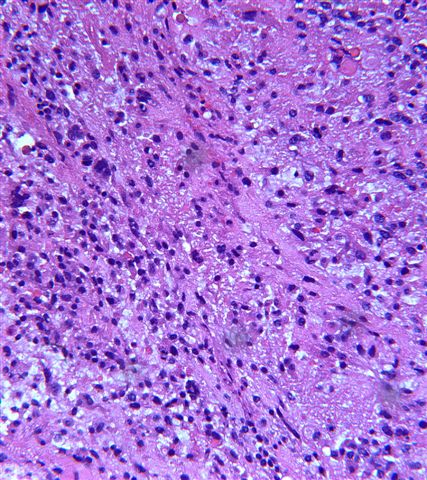
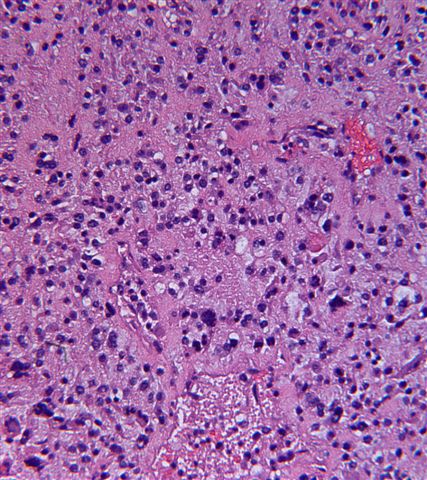
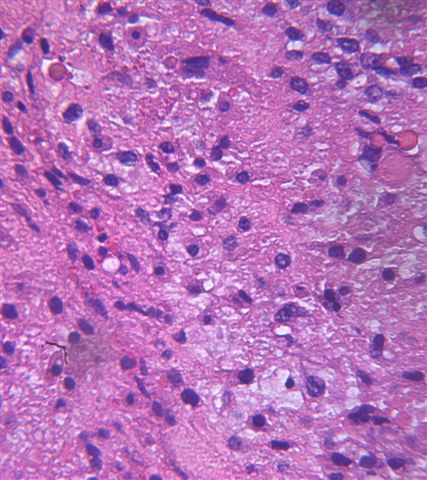
Undifferentiated embryonal sarcoma
Discussion:
Undifferentiated embryonal sarcoma comprises 10% of pediatric tumors, and is the third most common pediatric hepatic tumor after hepatoblastoma and hepatocellular carcinoma. It commonly occurs at ages 6 to 10 years, and only rarely occurs in adults (Cancer 2008;112:2274). It typically presents with pain, fever, an abdominal mass and a normal serum AFP (J Pediatr Surg 2008;43:1912).
Grossly, the tumor is up to 30 cm, well demarcated and soft, with cystic, gelatinous, hemorrhagic or necrotic foci. Histologically, it has variable cellularity, and is composed of anaplastic and spindle cells with ill defined borders and prominent PAS+ diastase resistant hyaline globules. The nuclei have stippled chromatin and indistinct nucleoli. The stroma has numerous thin walled vessels, and may be myxoid. There is frequent mitotic activity. The tumor periphery may demonstrate trapped hepatocytes or bile duct structures. Tumor cells are immunoreactive for vimentin with a high Ki-67 index, and negative for myogenin and keratin (Appl Immunohistochem Mol Morphol 2006;14:193). The hyaline globules are negative for alpha fetoprotein.
The differential diagnosis includes mesenchymal hamartoma (usually < 1 year old, cystic tumor with bland tumor cells and no giant cells), embryonal rhabdomyosarcoma (usually 2-6 years old, myxoid mass extending into bile duct, rhabdomyoblastic differentiation with cytoplasmic cross striations, cambium layer present but no diffuse anaplasia or hyaline globules, myogenin+, myoD1+, Pediatr Dev Pathol 2007;10:89), sarcomatoid hepatocellular carcinoma and a mixed form of hepatoblastoma. Hydatid cyst is also a consideration in endemic areas (J Pediatr Surg 2008;43:E1).
Treatment is complete resection and chemotherapy (J Gastrointest Surg 2007;11:73), and the prognosis is now considered good (Cancer 2002;94:252). Large tumors may rupture and cause death (J Pediatr Hematol Oncol 2007;29:63).
Nat Pernick, M.D., President
PathologyOutlines.com, Inc.
30100 Telegraph Road, Suite 408
Bingham Farms, Michigan (USA) 48025
Telephone: 248/646-0325
Email: NatPernick@Hotmail.com
Alternate email: NatPernick@gmail.com