
31 October 2008 Case of the Week
#133
To view the images or references,
you must click on the links in blue. Links in green are to journals with free full text-no
registration. You can also access these
cases by visiting our Home Page, then click on the Case of the
Week button on the left hand side.
This email is sent only to
subscribers. To subscribe or
unsubscribe, email NatPernick@Hotmail.com,
indicating subscribe or unsubscribe to Pathology Case of the Week. There is no charge. We do not sell, share or use your email
address for any other purpose. We also
have free email subscriptions for Pathologist/PhD jobs (biweekly), Other
laboratory jobs (biweekly), Pathology website news (monthly) and Pathology new
books (monthly). Email us to subscribe.

2nd Annual Winter Update in Clinical and
Laboratory Medicine:
Clinical Chemistry, Immunology, Microbiology and
Molecular Medicine
This 24 hour review and update in
the areas of clinical chemistry, immunology, microbiology, and molecular
medicine is intended to improve knowledge about the pathogenesis and clinical
manifestations of a wide variety of metabolic, infectious,
immunologic, and genetic disorders along with the selection,
performance, and interpretation of clinical laboratory tests.

Approximately 60% of the diagnoses
in medicine are based on the results of laboratory testing. The 2nd Annual Winter
Update program will address this major gap in knowledge and
inform the participant about developments in clinical laboratory testing and
their relevance to clinical medicine. The
conference is held at The Canyons in
How
can you learn about new fellowship openings?
We have a new email list sent out every two weeks, listing the new
fellowships posted at our website. To
subscribe, email NatPernick@Hotmail.com with subscribe
to Path fellowships email in the subject line.
We
have started a new section on Board Review
Questions. If you have sample questions and answers, just
email them to us.
Tell
your colleagues about our Other Laboratory Jobs
page, which includes jobs for PAs, cytotechs, med techs, histotechs, managers,
etc., and now includes related corporate jobs,
such as pathology related sales. If you
are looking to fill a position, the cost for these ads is only $500 for 6
months.
We thank Dr. Angela Bohlke,
Case of the Week #133
Clinical
History
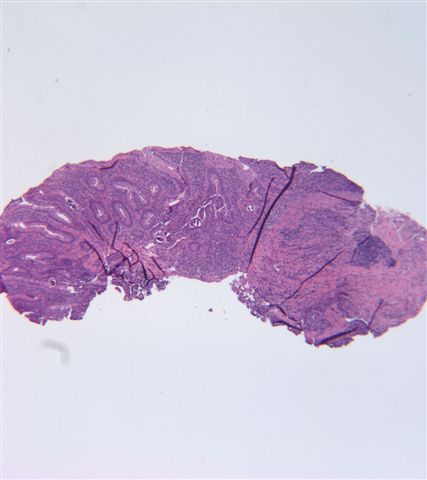
A 43 year-old Honduran man presented
with diarrhea and abdominal pain for one month. Physical findings and endoscopy were
unremarkable. Duodenal biopsies were
obtained.
{kind=link}
{kind=link}
{kind=link}
What is your diagnosis?
Diagnosis:
Strongyloides stercoralis
Discussion:
Subsequent stool findings showed
Strongyloides ova.
Strongyloides is a nematode whose
larvae buries into the mucosa of the duodenum and jejunum, where they mature
into adults. The females then lay eggs,
which develop into larvae that pass into the stool, where they mature and
become infective. The infective larvae penetrate
intact skin, usually through the feet. The
larvae enter the circulatory system, are transported to the lungs, and enter
the alveolar spaces. They then are
carried to the trachea and pharynx, are swallowed, and enter the intestinal
tract, where the process is repeated. If
the larvae become infective before leaving the body, they may invade the
intestinal mucosa or perianal skin, causing autoinfection (see life cycle).
Most patients suffer diarrhea,
malabsorption or no symptoms. Immunocompromised
individuals can acquire disseminated strongyloidiasis, a possibly fatal
condition in which worms move into other organs (WormBook 2007 May 23:1).
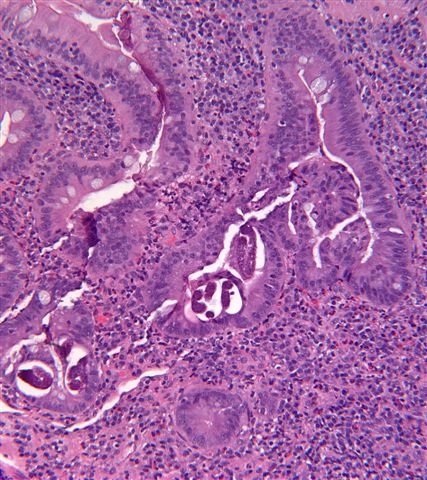
Diagnosis is by stool exam, looking
for larvae, or by biopsy of small intestinal mucosa, looking for the adult
female or eggs. There is often
granulomatous or eosinophilic inflammation.
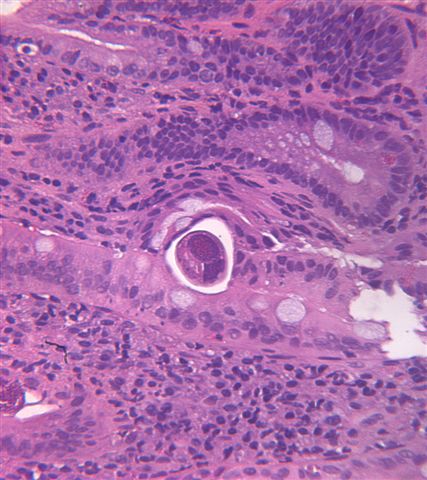
In female worms, the intestine or ovaries may
be prominent (image). In gravid females,
an egg (green arrow) may be identified within the uterus .
Treatment is with antihelminths,
such as thiabendazole (Ann Pharmacother 2007;41:1992). Prevention is by wearing shoes in endemic
areas.
Nat Pernick, M.D., President
PathologyOutlines.com, Inc.
Bingham Farms,
Telephone: 248/646-0325
Email: NatPernick@Hotmail.com
Alternate email: NatPernick@gmail.com