
22 October 2008 – Case of the Week #132
To view the images or references, you must click on the links in blue. Links in green are to journals with free full text-no registration. You can also access these cases by visiting our Home Page, then click on the Case of the Week button on the left hand side.
This email is sent only to subscribers. To subscribe or unsubscribe, email NatPernick@Hotmail.com, indicating subscribe or unsubscribe to Pathology Case of the Week. There is no charge. We do not sell, share or use your email address for any other purpose. We also have free email subscriptions for Pathologist/PhD jobs (biweekly), Other laboratory jobs (biweekly), Pathology fellowships (biweekly), Pathology website news (monthly) and Pathology new books (monthly). Email us to subscribe.

23rd Annual Park City Surgical Pathology Workshop
This 20-hour workshop is designed for the pathologist, clinician, and oncology specialist, focusing on surgical pathology, cytopathology, and hematopoietic pathology.
Short lectures and case-oriented discussions will include in-depth reviews of diagnostic anatomic pathology, insight into difficult differential diagnoses, use of immunohistochemistry and new technology to improve diagnosis.

Participants at the 23rd Annual Surgical Pathology Workshop will be asked to examine microscopic images and formulate a diagnosis and patient management strategy. The faculty pathologist will then discuss the diagnosis, differential diagnosis, patient management, and other pertinent features. Cases will be selected to represent common and/or difficult diagnostic problems. Held at The Canyons in Park City, Utah. Click here for our website.
We have two new email lists. First, every two weeks, we send subscribers a list of new fellowships posted at our website. To subscribe, email NatPernick@Hotmail.com with “subscribe to Path fellowships email” in the subject line. Second, we have a monthly email about our charity, The Detroit College Promise. To subscribe, email us with "subscribe to DCP news" in the subject line.
By request, we are adding a section on Board Review Questions. If you have sample questions and answers, just email them to us.
We have an Other Laboratory Jobs page, which includes PAs, cytotechs, med techs, histotechs, managers, etc., and now includes related corporate jobs, such as sales. The cost for these ads is $500 for 6 months.
We thank Dr. Daniel Ostler, MD Anderson Cancer Center, Houston, Texas (USA) for contributing this case. To contribute a Case of the Week, email NatPernick@Hotmail.com with the clinical history, your diagnosis and diagnostic microscopic images in JPG, GIF or TIFF format (send as attachments, we will shrink if necessary). Please include any other images (gross, immunostains, etc.) that may be helpful or interesting. We will write the discussion (unless you want to), list you as the contributor, and send you $35 (US dollars) by check or PayPal for your time after we send out the case. Please only send cases with high quality images and a diagnosis that is somewhat unusual (or a case with unusual features).
Case of the Week #132
Clinical History
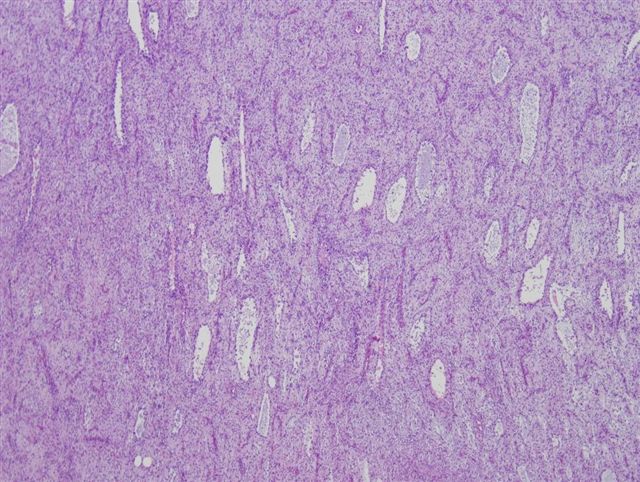
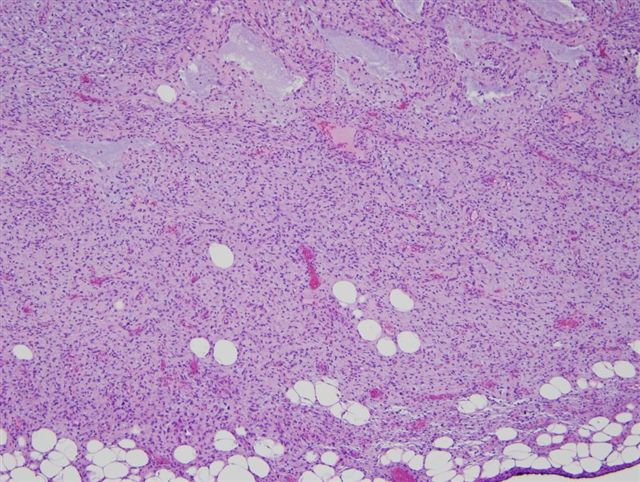
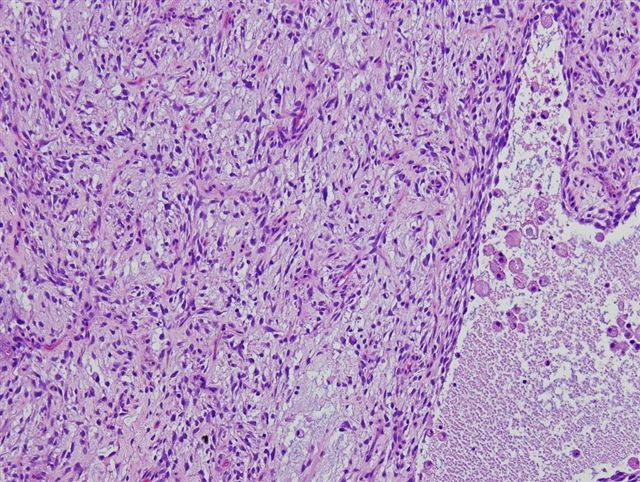
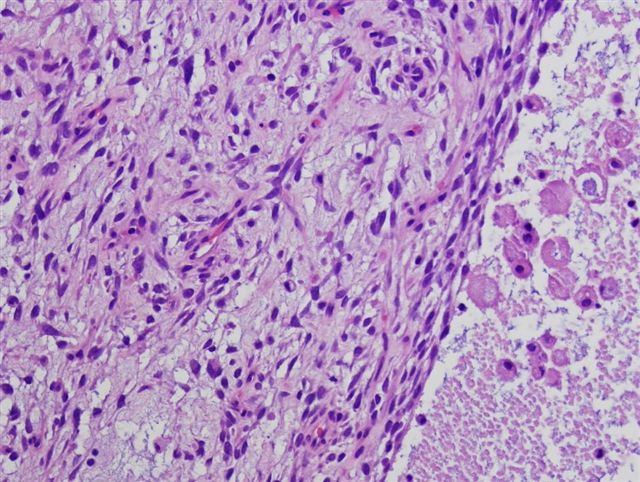
A 54 year old woman had a right supraclavicular mass, which clinically resembled a lymph node.
Micro images: #1; #2; #3; #4; #5
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
What is your diagnosis?
Diagnosis:
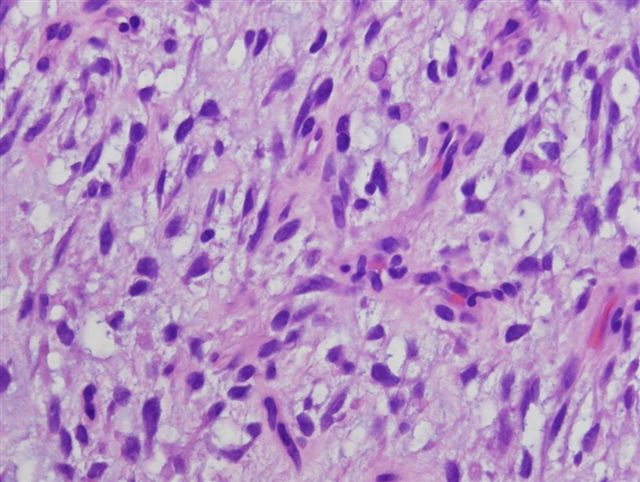
Dermatofibrosarcoma protuberans (DFSP), myxoid variant
Discussion:
The microscopic images show a sheet like proliferation of relatively bland spindle cells that infiltrate the adjacent fat, in a myxoid stroma. Numerous thin walled vessels are present. The spindle cells have pale eosinophilic cytoplasm and stellate nuclei without pleomorphism. The tumor cells were immunoreactive for CD34 (images not provided).
The myxoid variant of DFSP is defined as having at least 50% myxoid stroma. It is an uncommon variant, but has the same prognosis as classic DFSP (AJSP 2007;31:1371). The tumor cells are immunoreactive for CD34, and negative for S100 and muscle markers.
The differential diagnosis includes benign and malignant tumors. Myxoid neurofibroma has wavy nuclei, and often intratumoral axons. It is strongly S100 positive. Superficial angiomyxoma also has a myxoid stroma with numerous small vessels and may be CD34 positive. However, it does not infiltrate fat and tends to be less cellular. Myxoid liposarcoma has vessels that are more abundant, delicate and branching than the vessels of myxoid DFSP. In addition, lipoblasts are prominent.
Treatment of myxoid DFSP, like classic DFSP, consists of complete excision. The prognosis is good, with only occasional recurrences (Am J Dermatopathol 2007;29:443).
Nat Pernick, M.D., President
PathologyOutlines.com, Inc.
30100 Telegraph Road, Suite 408
Bingham Farms, Michigan (USA) 48025
Telephone: 248/646-0325
Email: NatPernick@Hotmail.com
Alternate email: NatPernick@gmail.com