
29 August 2008 – Case of the Week #128
To view the images or references, you must click on the links in blue. Links in green are to journals with free full text-no registration. You can also access these cases by visiting our Home Page, then click on the Case of the Week button on the left hand side.
This email is sent only to subscribers. To subscribe or unsubscribe, email NatPernick@Hotmail.com, indicating subscribe or unsubscribe to Pathology Case of the Week. There is no charge. We do not sell, share or use your email address for any other purpose. We also have free email subscriptions for Pathologist/PhD jobs (biweekly), Other laboratory jobs (biweekly), Pathology website news (monthly) and Pathology new books (monthly). Email us to subscribe.
Please tell your staff, residents and fellows about PathologyOutlines.com, and about our mailing lists. Also tell us how we can make this website more useful to you, by email (NatPernick@Hotmail.com), telephone (248/646-0325), or by stopping by our booths at the upcoming AAPA, CAP or ASCP meetings.
We thank Drs. Mona Kandil, Nancy Asaad and Asmaa Abdou, from Menofiya University, Egypt, for contributing this case. To contribute a Case of the Week, email NatPernick@Hotmail.com with the clinical history, your diagnosis and diagnostic microscopic images in JPG, GIF or TIFF format (send as attachments, we will shrink if necessary). Please include any other images (gross, immunostains, etc.) that may be helpful or interesting. We will write the discussion (unless you want to), list you as the contributor, and send you $35 (US dollars) by check or PayPal for your time after we send out the case. Please only send cases with high quality images and a diagnosis that is somewhat unusual (or a case with unusual features).
Case of the Week #128
Clinical History
A 29 year old man presented with left renal hydronephrosis by clinical exam and radiology. Since the kidney was nonfunctioning, it was excised.
Gross images: left kidney
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
What is your diagnosis?
Diagnosis:
Suggestive of renal tuberculosis
End stage kidney disease
Discussion:
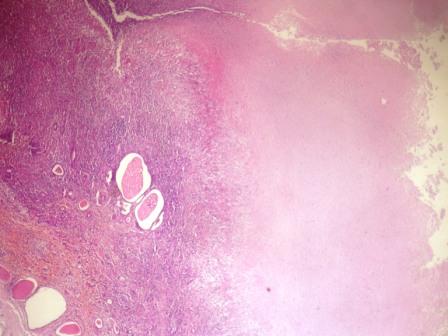
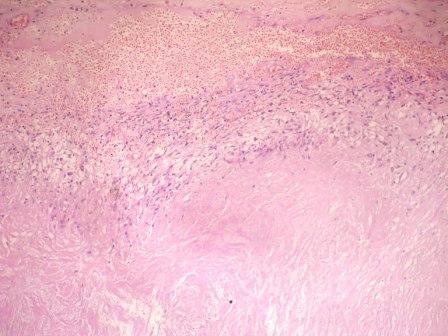
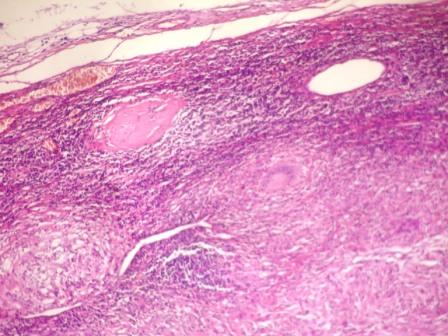
The kidney grossly had multiple cavities filled with yellow friable material. Microscopically, the renal parenchyma was compressed by extensive caseous necrosis, with occasional granulomas composed of epithelioid cells and Langhans giant cells. There was also cortical deposition of hyaline type material, suggestive of amyloid. Subsequently, the pathologists were informed that the patient had a chronic history of pulmonary tuberculosis. A culture was also positive for tuberculosis.
The World Health Organization estimates that 9 million new cases of tuberculosis disease occur each year, and that tuberculosis causes nearly 2 million annual deaths (WHO: Global Tuberculosis Control 2008). After the lungs, the genitourinary tract is the most common site of infection. Renal involvement may be indolent, and may not become apparent until 20+ years from detection of the primary infection.
Urogenital tuberculosis is associated with a unilateral non-functioning kidney in 27% of cases, with renal failure present in 7% (Int J Urol 2008 Jul 10 [Epub ahead of print]). Conversely, in chronic kidney disease of all causes, one study from India demonstrated a 4% incidence of tuberculosis, which was usually tuberculin skin test negative (Clin Nephrol 2007;67:217).
The differential diagnosis includes xanthogranulomatous pyelonephritis (Int J Urol 2006;13:67). It has a different clinical picture and lacks acid-fast bacilli, although they may be difficult to detect even in tuberculosis patients.
Nat Pernick, M.D., President
PathologyOutlines.com, Inc.
30100 Telegraph Road, Suite 404
Bingham Farms, Michigan (USA) 48025
Telephone: 248/646-0325
Email: NatPernick@Hotmail.com
Alternate email: NatPernick@gmail.com