
20 July 2008 Case of the Week #125
To view the images or references, you must click on the links in blue. Links in green are to journals with free full text-no registration. You can also access these cases by visiting our Home Page, then click on the Case of the Week button on the left hand side.
This email is sent only to subscribers. To subscribe or unsubscribe, email NatPernick@Hotmail.com, indicating subscribe or unsubscribe to Pathology Case of the Week. There is no charge. We do not sell, share or use your email address for any other purpose. We also have free email subscriptions for Pathologist/PhD jobs (biweekly), Other laboratory jobs (biweekly), Pathology website news (monthly) and Pathology new books (monthly). Email us to subscribe.

We have a new contest / drawing, open to anyone who works in a pathology department or laboratory. We will reimburse two winners the price plus shipping of any item purchased from Amazon.com, up to $50 (US), by check or PayPal. To be eligible:
● Visit Amazon.com through our website by clicking on the Amazon.com or aStore banners on our Home Page, Affiliates Page or above, or the Amazon.com links on our Books page. This tags your purchase as originating at our website.
● Purchase anything from Amazon.
● Fax (248/258-9147) or email (NatPernick@hotmail.com) us the confirmation of your purchase from Amazon. We need your email address from the confirmation so we can contact you if you win.
● Thats it! All purchases from 11 July 2008 through 31 December 2008 are eligible.
● You may enter more than once, but only one entry per week is eligible.
We thank Dr. Mowafak Hamodat, Eastern Health of Newfoundland and Labrador, St. Johns, Canada for contributing this case. This case was reviewed in May 2020 by Dr. Jennifer Bennett, University of Chicago and Dr. Carlos Parra-Herran, University of Toronto.
Case of the Week #125
Clinical History
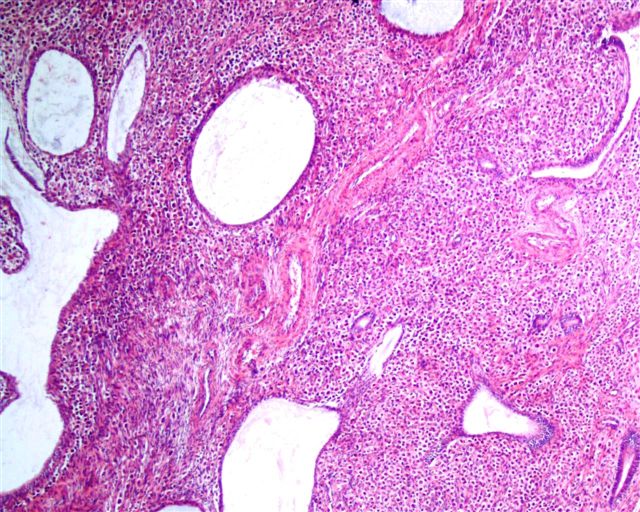
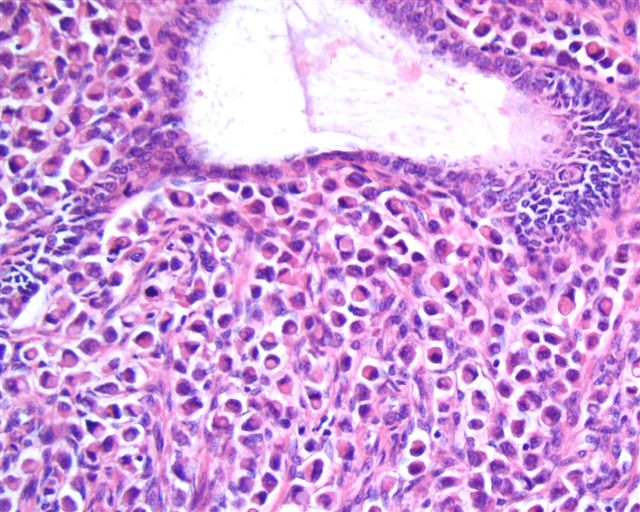
A 62 year old woman presented to her gynecologist with postmenopausal bleeding. Seven endometrial biopsies were taken, all showing negative results, although one was suggestive of an endometrial polyp. Physical examination showed uterine prolapse with cystocele, for which the patient requested a hysterectomy. Past medical history included well controlled hypertension, DVT and a mastectomy 12 years previous, for which she received Tamoxifen for a few years. A hysterectomy was performed. These sections are from an endometrial polyp.
{kind=link}
{kind=link}
{kind=link}
What is your diagnosis?
Diagnosis:
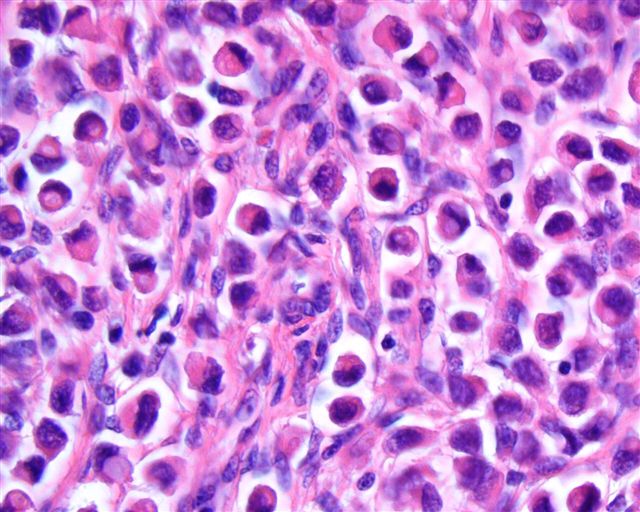
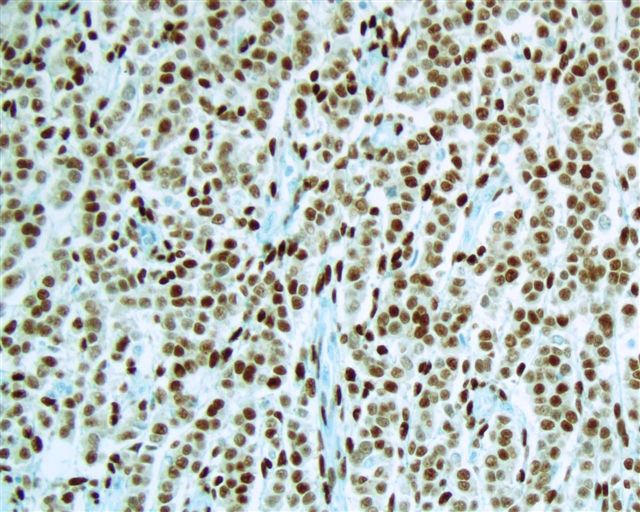
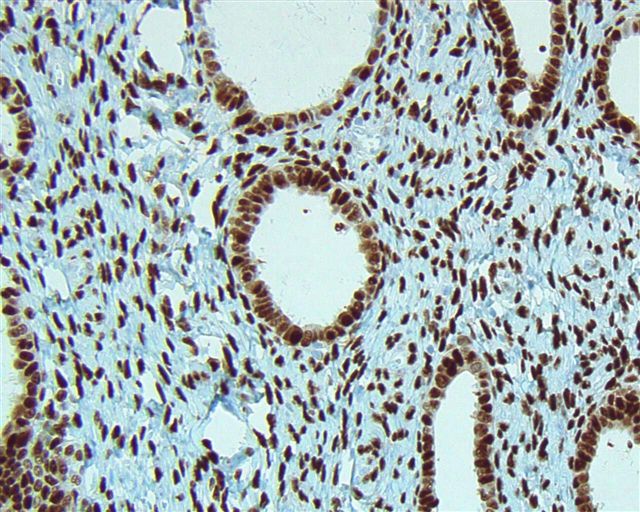
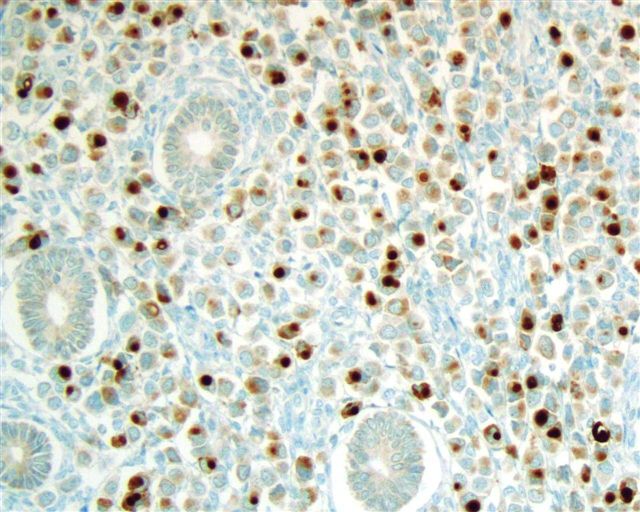
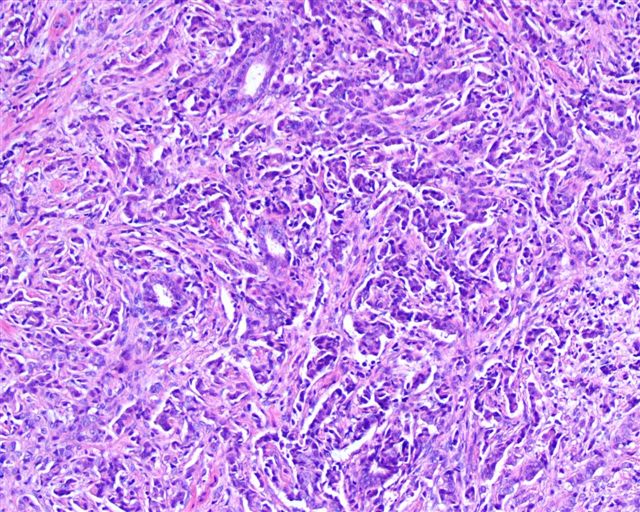
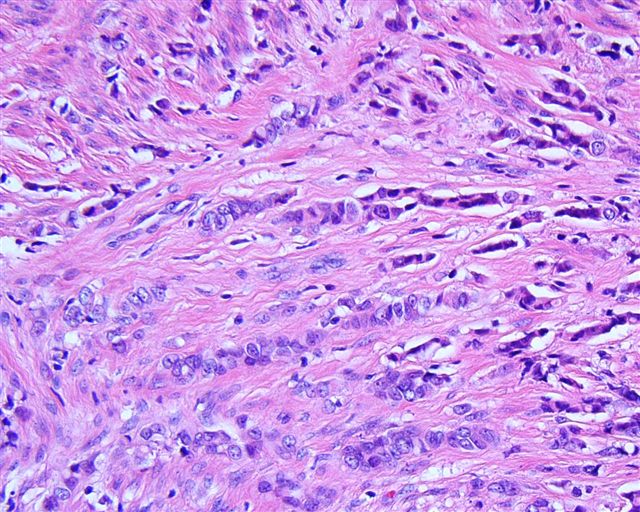
Metastatic lobular carcinoma in an endometrial polyp.
Discussion:
Immunostains were confirmatory for a breast metastasis (ER, PR, GCDFP-15). Metastases to the cervix (image #1; #2) were also identified, with a similar morphology and staining pattern. The mastectomy was apparently performed for lobular breast carcinoma, although no reports or slides were available.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Tamoxifen is an estrogen antagonist widely used for treatment or prevention of breast carcinoma. It may cause endometrial proliferative abnormalities, including endometrial polyps (Obstet Gynecol 1992;79:111). Since metastatic breast carcinoma to tamoxifen-associated polyps has been reported, usually involving lobular carcinoma (Ann Diagn Pathol 2005;9:166, Mod Path 2003;16:395, Gynecol Oncol 2005;97:946, Obstet Gynecol 2003;102:1149, Acta Obstet Gynecol Scand 1993;72:585), careful histologic evaluation of the endometrium is crucial in these patients.
Nat Pernick, M.D., President
PathologyOutlines.com, Inc.
30100 Telegraph Road, Suite 404
Bingham Farms, Michigan (USA) 48025
Telephone: 248/646-0325
Email: NatPernick@Hotmail.com
Alternate email: NatPernick@gmail.com