
20 June 2008 – Case of the Week #123
To view the images or references, you must click on the links in blue. Links in green are to journals with free full text-no registration. You can also access these cases by visiting our Home Page, then click on the Case of the Week button on the left hand side.
This email is sent only to subscribers. To subscribe or unsubscribe, email NatPernick@Hotmail.com, indicating subscribe or unsubscribe to Case of the Week. There is no charge. We do not sell, share or use your email address for any other purpose. We also have free email subscriptions for Pathologist/PhD jobs (biweekly), Other laboratory jobs (biweekly), website news (monthly) and new books (monthly). Email us to subscribe.
We thank Dr. Oscar Sanabria Monney, National Children’s Hospital, San Jose, Costa Rica, for contributing this case and part of the discussion. To contribute a Case of the Week, email NatPernick@Hotmail.com with the clinical history, your diagnosis and microscopic images in JPG, GIF or TIFF format (send as attachments, we will shrink if necessary). Please include any other images (gross, immunostains, etc.) that may be helpful or interesting. We will write the discussion (unless you want to), list you as the contributor, and send you $35 (US dollars) by check or PayPal for your time after we send out the case. Please only send cases with high quality images and a diagnosis that is somewhat unusual (or a case with unusual features).
Do you have images of breast cancer specimens that are post-tamoxifen or other hormonal therapy? We are updating our Breast malignant chapter, and images or publications regarding these changes would be helpful. Contact Dr. Pernick by phone or email below.
Case of the Week #123
Clinical History
A 1 year old boy had a slow growing cervical mass for 8 months, with recent laryngeal stridor.
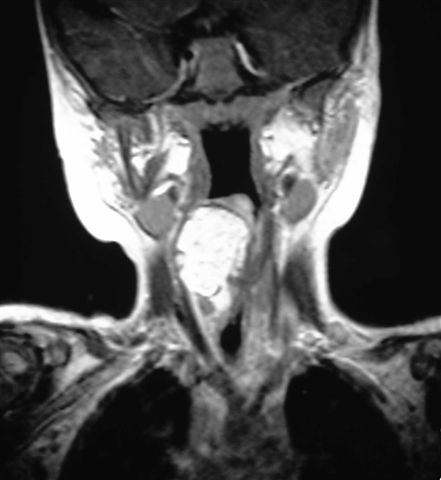
A neck ultrasound showed a solid homogenous retropharyngeal mass that pushed against the trachea. MRI identified a 3 x 2 cm mass with the density of fatty tissue (image). A fine needle aspiration and excision were performed.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
What is your diagnosis?
Diagnosis:
Lipoblastoma
Discussion:
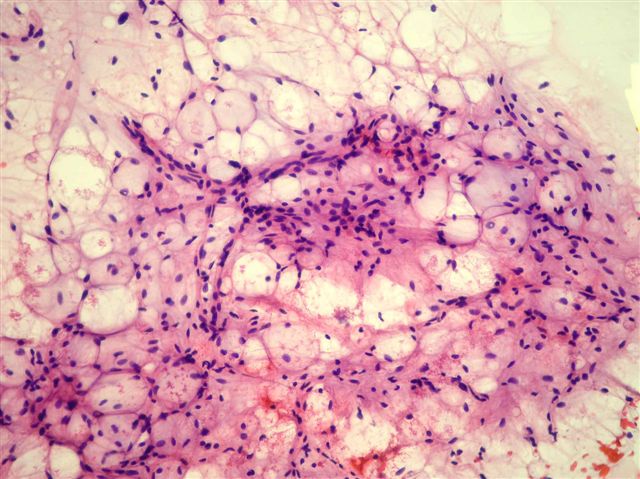
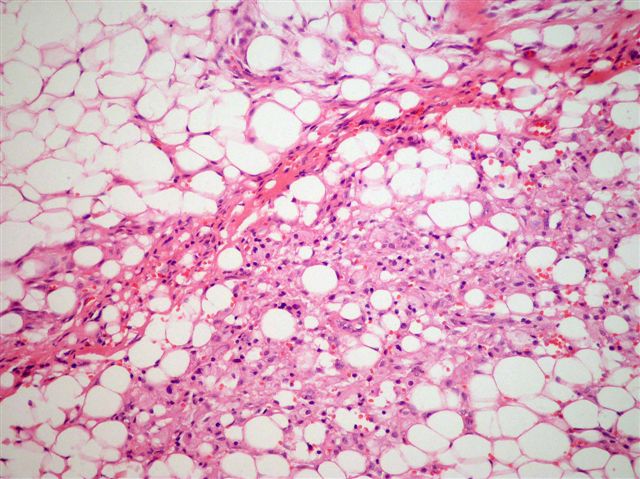
Cytologic smears showed fragments of mature adipose tissue with occasional vacuolated adipocytes (lipoblasts), in a myxoid stroma. The cells have centrically located small nuclei, without indentations. No necrosis, atypia or mitotic figures were present. Cytologic features are suggestive of lipoblastoma, although the differential diagnosis also includes lipoma with regressive changes, well-differentiated liposarcoma and myxoid liposarcoma. In addition to the cytologic features, the patient's age is very useful (Diagn Cytopathol 2005;33:195)
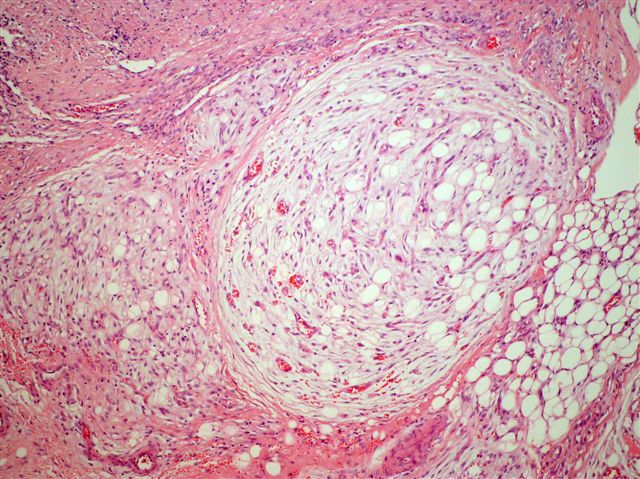
Lipoblastoma is a benign and uncommon tumor of adipose tissue that occurs primarily in young children, usually age 5 years or younger (AJSP 1997;21:1131). It resembles fetal adipose tissue, with lobules of immature fat cells that are separated by fibrous septa and myxoid matrix. Chromosome 8q11-13 is rearranged in 82% (Cancer Genet Cytogenet 2008;183:60), which includes the PLAG1 gene (Am J Pathol 2001;159:955). FISH may be helpful to confirm the diagnosis (Histopathology 2008;52:294).
The differential diagnosis includes myxoid liposarcoma and well-differentiated liposarcoma. Myxoid liposarcoma is rare before age 10 years, and is commonly associated with t(12;16)(q13;p11). It has no distinct lobulation, and often has nuclear atypia, mitotic figures, hyperchromasia and hypercellularity. Well differentiated liposarcoma is also rare in children. It has mature fat but no lipoblasts. It contains spindle cells with large, deep-staining nuclei and marked nuclear enlargement or pleomorphism; cellularity is low. MDM2 and CDK4 immunostains are sensitive and specific markers (AJSP 2005;29:1340).
Complete excision of lipoblastoma is the treatment of choice. The diffuse form (lipomatosis) can be difficult to excise completely, which may lead to recurrence. Follow up for 3 years or more is recommended (Pediatr Surg Int 2005;21:809).
References: PathologyOutlines.com - Soft Tissue Tumors Part 1-Intro, Fibrous, Fibrohistiocytic and Adipose
Nat Pernick, M.D., President
PathologyOutlines.com, Inc.
30100 Telegraph Road, Suite 404
Bingham Farms, Michigan (USA) 48025
Telephone: 248/646-0325
Email: NatPernick@Hotmail.com
Alternate email: NatPernick@gmail.com