
13 June 2008 Case of the Week #122
To view the images or references, you must click on the links in blue. Links in green are to journals with free full text-no registration. You can also access these cases by visiting our Home Page, then click on the Case of the Week button on the left hand side.
This email is sent only to subscribers. To subscribe or unsubscribe, email NatPernick@Hotmail.com, indicating subscribe or unsubscribe to Case of the Week. There is no charge. We do not sell, share or use your email address for any other purpose. We also have free email subscriptions for Pathologist/PhD jobs (biweekly), Other laboratory jobs (biweekly), website news (monthly) and new books (monthly). Email us to subscribe.

Attend the
Annual Summer Update in Clinical Immunology,
Microbiology and Infectious Diseases
July 14-18, 2008
Snow King Resort
Jackson, Wyoming (USA)

This 25.75-hour review and update in clinical immunology, microbiology and infectious diseases is intended to improve knowledge about the pathogenesis and clinical manifestations of infectious diseases, immunological mechanisms of disease and disease prevention, appropriate approaches to the diagnosis of infections and immunologic disorders, and utilization of the clinical microbiology and immunology laboratory, including selection and interpretation of results.
This course will provide a forum for the exchange of ideas dealing with microbial infections as well as immunity to infectious diseases and immunologic disorders.
For more information or to register, please click here.
Visit and use our newly updated chapter - Soft Tissue Tumors-Part 1 (link is also in the center section of our Home Page). It starts with approaches to diagnosis, syndromes, grading and molecular patterns. It then discusses all known fibroblastic / myofibroblastic, fibrohistiocytic and lipomatous tumors, include WHO and non-WHO entities (the remaining soft tissue tumors are discussed in the Soft Tissue Tumors-Part 2 chapter). Each entity contains an extensive discussion of clinical, gross, micro, stains and molecular features. Use the 1000+ high quality image links in this chapter to assist with signout, to educate other physicians or for preparing talks.
We thank Dr. R. F. Chinoy, Tata Memorial Hospital, Parel, Mumbai (India) for contributing this case. To contribute a Case of the Week, email NatPernick@Hotmail.com with the clinical history, your diagnosis and microscopic images in JPG, GIF or TIFF format (send as attachments, we will shrink if necessary). Please include any other images (gross, immunostains, etc.) that may be helpful or interesting. We will write the discussion (unless you want to), list you as the contributor, and send you $35 (US dollars) by check or PayPal for your time after we send out the case. Please only send cases with high quality images and a diagnosis that is somewhat unusual (or a case with unusual features).
Case of the Week #122
Clinical History
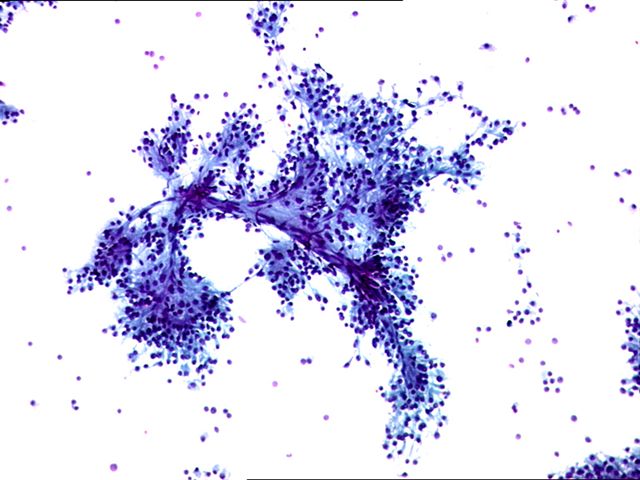
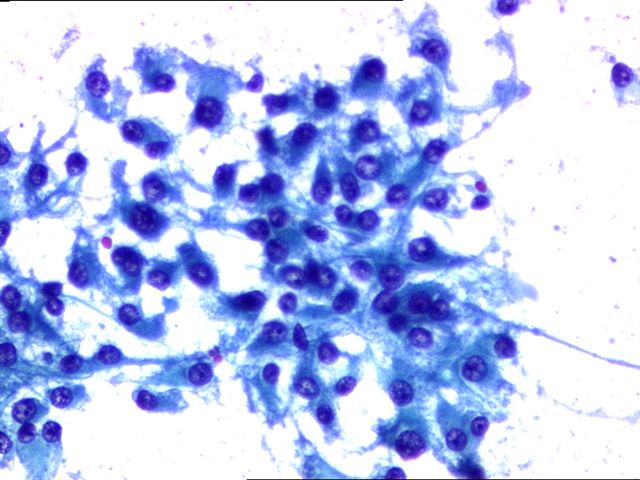
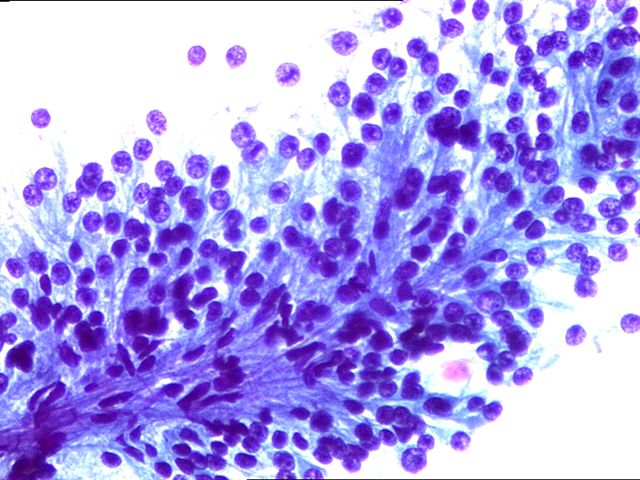
A 43 year old man presented with a painless testicular mass and normal serum AFP and beta-hCG. Fine needle aspiration cytology was followed by orchiectomy.
The tumor was 2.5 cm, tan brown and soft. The mass was within the testicular
parenchyma.
Cytology images: #1; #2; #3
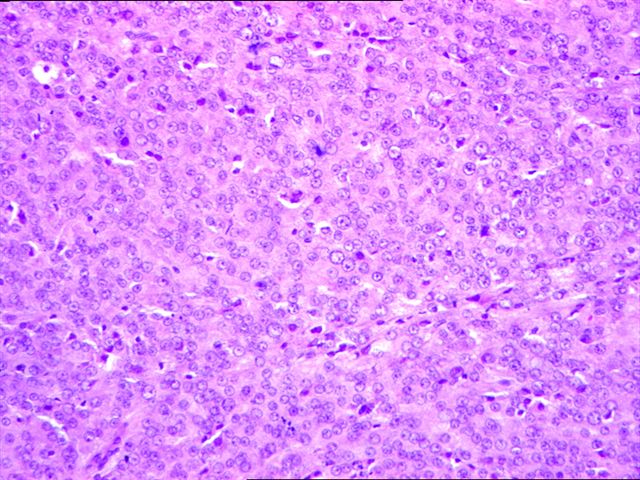
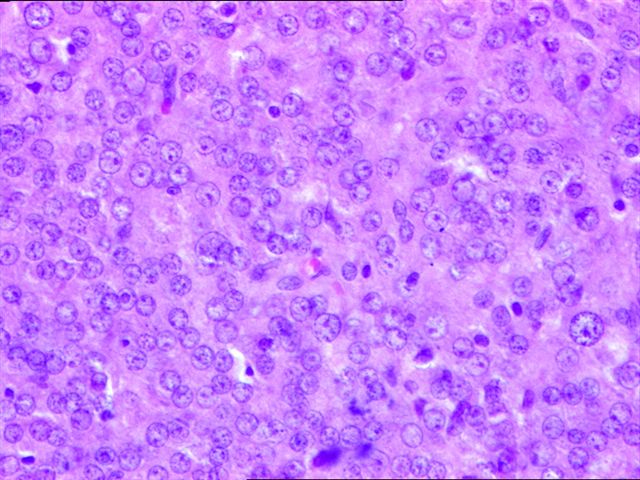
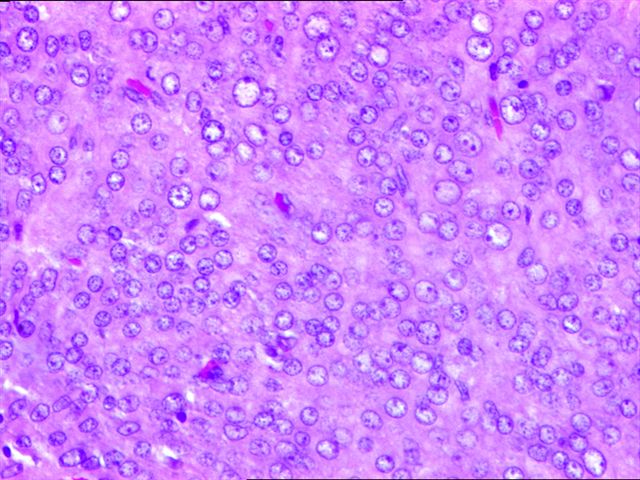
Micro images: #1; #2; #3; #4
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
What is your diagnosis?
Diagnosis:
Leydig cell tumor of the testes
Discussion
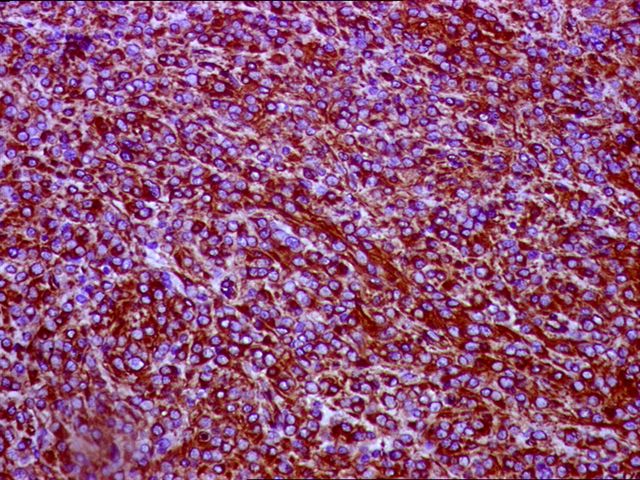
An inhibin stain was diffusely and strongly positive (image).
{kind=link}
Leydig cell tumors comprise 1-3% of testicular tumors. Although they arise at any age, most patients are 20-60 years old. They often secrete androgens, estrogens or corticosteriods, and patients may present with gynecomastia or other feminizing symptoms (Hum Path 1977;8:621), or with precocious puberty without spermatocytic maturation.
Grossly, the tumor is usually a solid, well circumscribed nodule 5 cm or less, with a distinct golden-brown homogenous cut surface. Up to 10% have extratesticular extension. Microscopically, there are sheets, nests, ribbons or cords of large, round or polygonal cells with defined cell borders, eosinophilic cytoplasm and round central nuclei. The cytoplasm may contain vacuoles, lipofuscin or Reinke crystals (35%). The tumor cells may display endocrine atypia. Occasionally, cells may have adipose differentiation, which should not be confused with extratesticular extension (AJSP 2002;26:1424). There is no/rare mitotic activity.
Positive immunostains include inhibin, MelanA and keratin, as well as vimentin and steroid hormones. Tumor cells are negative for S100.
The differential diagnosis includes nodular Leydig cell hyperplasia (associated with cryptorchidism, usually 1 cm or less, multifocal, does not destroy surrounding tubules), Large cell calcifying Sertoli cell tumor (usually multifocal, often bilateral, more stroma, calcifications, intratubular growth, no Reinkes crystals, slightly different immunostaining pattern, Pathol Int 2005;55:366) and testicular tumors of adrenogenital syndrome (bilateral, multifocal, clinical symptoms, laboratory findings, shrink after corticosteroid therapy)
Orchiectomy is usually curative for benign tumors, although testis-sparing surgery has also been advocated for young men (Int J Clin Pract 2003;57:912). In adults, 10% of tumors have malignant behavior, with metastases to lymph nodes, lung and liver. These tumors are usually > 5 cm with necrosis, vascular invasion, nuclear atypia, numerous mitoses including atypical ones, and infiltrative margins.
References: Archives 2007;131:311, AJSP 1985;9:177, eMedicine
Nat Pernick, M.D., President
PathologyOutlines.com, Inc.
30100 Telegraph Road, Suite 404
Bingham Farms, Michigan (USA) 48025
Telephone: 248/646-0325
Email: NatPernick@Hotmail.com
Alternate email: NatPernick@gmail.com